PDF - GJIDCR 2 106
PDF - GJIDCR 2 106
Download as pdf or txt
You might also like
- Three's A Crowd Final DraftDocument34 pagesThree's A Crowd Final DraftRyan Fortier95% (19)
- Full Download PDF of Test Bank For PSYCH 6th Edition Rathus All ChapterDocument63 pagesFull Download PDF of Test Bank For PSYCH 6th Edition Rathus All Chapterabdouhlosson0100% (9)
- RNR 4101 Management PlanDocument21 pagesRNR 4101 Management Planapi-522084028No ratings yet
- Acute Inflammation Robbins Basic Pathology Inflammation Repair PDFDocument24 pagesAcute Inflammation Robbins Basic Pathology Inflammation Repair PDFJessica Bittar Camargo100% (1)
- Distribution Channel ManagementDocument9 pagesDistribution Channel ManagementsujeetleopardNo ratings yet
- 17-07 - Salesforce Plus Adapter Administrator's GuideDocument175 pages17-07 - Salesforce Plus Adapter Administrator's GuideguillermoNo ratings yet
- Future Series - Future 2005.enDocument43 pagesFuture Series - Future 2005.enSteveAbonyi0% (1)
- Inflammatory Mechanisms: The Molecular Basis of Inflammation and DiseaseDocument7 pagesInflammatory Mechanisms: The Molecular Basis of Inflammation and DiseaseMaximeNo ratings yet
- From Inflammation To Sickness Historical PerspectiveDocument5 pagesFrom Inflammation To Sickness Historical PerspectiveВладимир ДружининNo ratings yet
- Molecular and Cellular Mechanisms of Inflammation: D. V. Kuprash and S. A. NedospasovDocument3 pagesMolecular and Cellular Mechanisms of Inflammation: D. V. Kuprash and S. A. NedospasovFo Chang (Lo)No ratings yet
- Inate InmunoterapyDocument22 pagesInate Inmunoterapyalex garciaNo ratings yet
- Source:Immunology Eight Edition David MaleDocument3 pagesSource:Immunology Eight Edition David MaleAzzahra FadhlilaNo ratings yet
- CYTOKINESDocument19 pagesCYTOKINESLatif Ahmad DarNo ratings yet
- Review Article: Role of Antioxidants and Natural Products in InflammationDocument15 pagesReview Article: Role of Antioxidants and Natural Products in InflammationMI SsouNo ratings yet
- Sistem ImunDocument24 pagesSistem ImundliaaNo ratings yet
- NIH Public Access: Author ManuscriptDocument29 pagesNIH Public Access: Author ManuscriptFifth TsuchikageNo ratings yet
- Immunology Unveiled: A Comprehensive Journey through the Human Immune System: Guardians of the Body: The Unseen Heroes of ImmunityFrom EverandImmunology Unveiled: A Comprehensive Journey through the Human Immune System: Guardians of the Body: The Unseen Heroes of ImmunityNo ratings yet
- Pathophysiology Septic ShockDocument26 pagesPathophysiology Septic ShockTinea Sycillia100% (1)
- Practica #9Document6 pagesPractica #9Pokemongo3478No ratings yet
- FR Robinns Inflammation & Repair F22 2Document12 pagesFR Robinns Inflammation & Repair F22 2GrantNo ratings yet
- Lecture Note On Basic ImmunologyDocument23 pagesLecture Note On Basic ImmunologyDavidsonNo ratings yet
- InflammationDocument117 pagesInflammationPraiseNo ratings yet
- Prologue Syllabus 2008Document14 pagesPrologue Syllabus 2008Francisco Eriberto de LimaNo ratings yet
- Treatment of Endodontic Infections-109-157Document49 pagesTreatment of Endodontic Infections-109-157Kirana YosandraNo ratings yet
- Vaccine Immunology: Understanding Modern Vaccines: Perspectives in VaccinologyDocument35 pagesVaccine Immunology: Understanding Modern Vaccines: Perspectives in VaccinologyYulinda AswanNo ratings yet
- Towards A Conceptual Framework For Innate ImmunityDocument14 pagesTowards A Conceptual Framework For Innate ImmunityEnrique PeironeNo ratings yet
- Artigo APG 11Document17 pagesArtigo APG 11Jose FragosoNo ratings yet
- 47.1 Nonspecific Defenses: Chapter 47: The Body's Defense SystemsDocument19 pages47.1 Nonspecific Defenses: Chapter 47: The Body's Defense Systemsapi-520057338No ratings yet
- Tinywow Inflammation 17791543Document117 pagesTinywow Inflammation 17791543Chidera EmmanuelNo ratings yet
- Acute InflammationDocument10 pagesAcute InflammationLydia Angel HartonoNo ratings yet
- Molecular Basis of Inflammation As Immune ResponseDocument7 pagesMolecular Basis of Inflammation As Immune ResponseFati MaNo ratings yet
- ImmunologyDocument38 pagesImmunologyquaisherhossainNo ratings yet
- Immunity Against Fungal Infections: Shuai JiangDocument4 pagesImmunity Against Fungal Infections: Shuai JiangShafira AzzahraNo ratings yet
- Phases of Acute Inflammation: Peradangan AkutDocument10 pagesPhases of Acute Inflammation: Peradangan AkutKesyaNo ratings yet
- 978 81 322 2680 2 - Chapter - 4Document41 pages978 81 322 2680 2 - Chapter - 4enjoy death eat your miojoNo ratings yet
- Role of Cytokines in Sepsis 2Document95 pagesRole of Cytokines in Sepsis 2ammar aboghalionNo ratings yet
- Blrincon - Bacterias Inmune ResponseDocument9 pagesBlrincon - Bacterias Inmune ResponseDavidf VillabonaNo ratings yet
- Introductiontothe Immune SystemDocument25 pagesIntroductiontothe Immune SystemUyên HuỳnhNo ratings yet
- Immunomodulatory Effects of Probiotics in The Intestinal TractDocument19 pagesImmunomodulatory Effects of Probiotics in The Intestinal TractputrinaraheswariNo ratings yet
- Immune System A Target For Functional FoodsDocument12 pagesImmune System A Target For Functional FoodsjenniNo ratings yet
- The Immune System: Lindsay B. NicholsonDocument27 pagesThe Immune System: Lindsay B. NicholsonAlanakimiNo ratings yet
- Sysmex SEED Haematology InflammatoryDocument7 pagesSysmex SEED Haematology InflammatoryTzeto Han CongNo ratings yet
- Pathophysiology of SepsisDocument8 pagesPathophysiology of SepsisntnquynhproNo ratings yet
- Ijms 24 01526 v2Document25 pagesIjms 24 01526 v2della.ps2310No ratings yet
- Chapter 1 - OverviewDocument47 pagesChapter 1 - OverviewZea Mae AgirNo ratings yet
- Therapeutic Application of Exosomes in Inflammatory DiseasesDocument22 pagesTherapeutic Application of Exosomes in Inflammatory Diseasessebass.tjacoboNo ratings yet
- Protection From HIV/AIDS: The Importance of Innate Immunity: Jay A. Levy, Iain Scott, and Carl MackewiczDocument8 pagesProtection From HIV/AIDS: The Importance of Innate Immunity: Jay A. Levy, Iain Scott, and Carl MackewiczSofi Papel JachoNo ratings yet
- Cytoquine Storm and SepsisDocument12 pagesCytoquine Storm and SepsisEduardo ChanonaNo ratings yet
- Sepsis PatofisiologiDocument9 pagesSepsis Patofisiologiinstalasi farmasi rsu bangliNo ratings yet
- Balin 2018Document13 pagesBalin 2018Murti NopitasariNo ratings yet
- Immuno-Virology-Bacteriology Book Version 103Document332 pagesImmuno-Virology-Bacteriology Book Version 103Goose ChapmanNo ratings yet
- Immunology Science and Public Health TheDocument1 pageImmunology Science and Public Health ThezishidayatullahbatamNo ratings yet
- 10 1056@NEJMra1911109 PDFDocument11 pages10 1056@NEJMra1911109 PDFMартин ДончевNo ratings yet
- InflammationDocument83 pagesInflammationpriyaNo ratings yet
- Pathology (Inflammation and Wound Healing)Document14 pagesPathology (Inflammation and Wound Healing)andrew100% (1)
- Nature 06246Document8 pagesNature 06246Hagar AlaaNo ratings yet
- Inflammation and Inflammatory MediatorsDocument28 pagesInflammation and Inflammatory Mediatorsla.instagramawaNo ratings yet
- The Metabolic Basis of Immune Dysfunction Following Sepsis and TraumaDocument21 pagesThe Metabolic Basis of Immune Dysfunction Following Sepsis and TraumaJulia AlmeidaNo ratings yet
- +2 Bio-Zoo-Em 7-12Document30 pages+2 Bio-Zoo-Em 7-12aj techNo ratings yet
- Section 2 ImmunologyDocument14 pagesSection 2 ImmunologyricardoNo ratings yet
- Immune Responses To Human Papillomavirus: Margaret StanleyDocument7 pagesImmune Responses To Human Papillomavirus: Margaret StanleyDina A. ŠabićNo ratings yet
- Introduction To Immunology PDFDocument15 pagesIntroduction To Immunology PDFanon_143800659100% (1)
- Contribution of CD8+ T Cells To Control of Mycobacterium Tuberculosis InfectionDocument20 pagesContribution of CD8+ T Cells To Control of Mycobacterium Tuberculosis InfectionhelmiprasNo ratings yet
- Cdi2008 639803Document20 pagesCdi2008 639803Miguel RuizNo ratings yet
- Comprehensive Insights into Acute Cutaneous Lupus: Unraveling Pathways, Implications, and InterventionsFrom EverandComprehensive Insights into Acute Cutaneous Lupus: Unraveling Pathways, Implications, and InterventionsNo ratings yet
- Tapia, Charevie 3Document4 pagesTapia, Charevie 3rcdcaviteNo ratings yet
- The Effects of The Juvenile Draft 2Document9 pagesThe Effects of The Juvenile Draft 2api-403930494No ratings yet
- IO SCRIPT Jai Agarwal NEWDocument2 pagesIO SCRIPT Jai Agarwal NEWjaiNo ratings yet
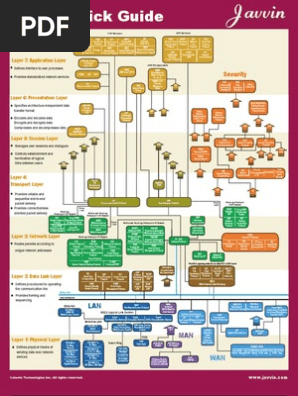
- TCP IP Quick GuideDocument4 pagesTCP IP Quick GuideDinh Truong Cong100% (1)
- Grains of Truth About: BagelsDocument2 pagesGrains of Truth About: Bagelsgeo_gabe_galan5473No ratings yet
- Research Paper On 3g Vs WifiDocument7 pagesResearch Paper On 3g Vs Wifieffbd7j4100% (1)
- TF Better Performance With TF - FunctionDocument5 pagesTF Better Performance With TF - FunctionRodrigoCastellanoNo ratings yet
- B.A (Hons) Political Sceince Colonialism in India Sem-I (7230)Document2 pagesB.A (Hons) Political Sceince Colonialism in India Sem-I (7230)diksha joshiNo ratings yet
- Crowd Estimation of The Black Nazarene Procession in Manila, PhilippinesDocument11 pagesCrowd Estimation of The Black Nazarene Procession in Manila, PhilippinesDuc Trung Vu CssrNo ratings yet
- HihiDocument20 pagesHihiCath OquialdaNo ratings yet
- Love and Dejection, Just Fiction EditionDocument55 pagesLove and Dejection, Just Fiction EditionImran NazeerNo ratings yet
- Pier 8 Arrastre & Stevedoring Services, Inc. vs. Confesor, G.R. No. 110854, February 13, 1995, 214 SCRA 295Document16 pagesPier 8 Arrastre & Stevedoring Services, Inc. vs. Confesor, G.R. No. 110854, February 13, 1995, 214 SCRA 295jonbelzaNo ratings yet
- Utu (Shamash)Document6 pagesUtu (Shamash)Ljubomir LukićNo ratings yet
- Tds Coa Msds Cek List Cas No. Inci Name: DMDM Hydantoin 6440-58-0Document1 pageTds Coa Msds Cek List Cas No. Inci Name: DMDM Hydantoin 6440-58-0rabbindra gustavNo ratings yet
- PSS SINCAL 16.0: Multiple FaultsDocument25 pagesPSS SINCAL 16.0: Multiple FaultsAntonio Olmedo AvalosNo ratings yet
- Communicative CompetenceDocument2 pagesCommunicative CompetenceErick TrilloNo ratings yet
- Analisis Perspektif Mahasiswa Pada Penerapan Kertas Kerja Atlas (Audit Tool and Linked Archive System)Document5 pagesAnalisis Perspektif Mahasiswa Pada Penerapan Kertas Kerja Atlas (Audit Tool and Linked Archive System)Riyan PramudiyaNo ratings yet
- Platts Methodology and Specifications Guide - Asian Oil ProductsDocument25 pagesPlatts Methodology and Specifications Guide - Asian Oil ProductsSun QianNo ratings yet
- LIVRO-Film-Architectureand Transnational Imagination Set Design in 30sDocument320 pagesLIVRO-Film-Architectureand Transnational Imagination Set Design in 30sAna Paola OttoniNo ratings yet
- TPT - Playdough Mats - The Human BodyDocument14 pagesTPT - Playdough Mats - The Human BodyFELIPE ANDRES100% (1)
- English Olympiad Level 3: Sections Q1 Q2 Q3 Q4 Q5 Q6 Q7 Q8 Q9 Q10 Q11 Q12 Q13 Total Marks ObtainedDocument6 pagesEnglish Olympiad Level 3: Sections Q1 Q2 Q3 Q4 Q5 Q6 Q7 Q8 Q9 Q10 Q11 Q12 Q13 Total Marks ObtainednkhsrNo ratings yet
- 03 9709 12 MS Prov Rma 08022023110949Document15 pages03 9709 12 MS Prov Rma 08022023110949Erven FernandesNo ratings yet
- OHSMS - Delegate Activity Manual - LA - NOV-2022-SARAS - CopieDocument33 pagesOHSMS - Delegate Activity Manual - LA - NOV-2022-SARAS - CopieZakaria Zéko BennaouiNo ratings yet
- WSF Outline TodayDocument3 pagesWSF Outline TodayOyekeye GokeNo ratings yet