Porphyria
21 likes8,738 views
Porphyria is caused by deficiencies in enzymes involved in heme biosynthesis, leading to accumulation of porphyrins and their precursors. There are several types of porphyria classified by enzyme deficiency, symptoms, or origin of excess precursors. Acute porphyrias involve neurologic or abdominal symptoms, while cutaneous porphyrias cause skin problems when exposed to sunlight. Porphyria results from partial deficiencies in enzymes that are sufficient under normal conditions but can be exacerbated by external factors, causing intermediates to accumulate and spill over.
























More Related Content
What's hot (20)
Similar to Porphyria (20)
More from Dinoosh De Livera (20)
Recently uploaded (20)
Porphyria
- 1. {{ Porphyria:Porphyria: etiology, pathogenesis, morphology,etiology, pathogenesis, morphology, causes of the death.causes of the death. Dinoosh De LiveraDinoosh De Livera Doctor InternDoctor Intern Vitebsk State Medical UniversityVitebsk State Medical University BelarusBelarus
- 2. Patients with porphyria pass urine that, onPatients with porphyria pass urine that, on standing, acquires astanding, acquires a port wine colour – theport wine colour – the name porphyria is derived from the Greekname porphyria is derived from the Greek ‘porphuros’ meaning red/purple.‘porphuros’ meaning red/purple. The porphyrias are caused by deficiencies of enzymes involved inThe porphyrias are caused by deficiencies of enzymes involved in heme biosynthesis which lead to blockade of the porphyrinheme biosynthesis which lead to blockade of the porphyrin pathway and subsequent accumulation ofpathway and subsequent accumulation of porphyrins and theirporphyrins and their precursors.precursors. Introduction:Introduction:
- 3. Porphyrins are heterocyclic organic compounds (non-protein portionPorphyrins are heterocyclic organic compounds (non-protein portion ofof hemoglobin) play vital role in heme-biosynthesis & are normal body chemicals,hemoglobin) play vital role in heme-biosynthesis & are normal body chemicals, generally do not accumulate.generally do not accumulate. Porphyrins are essential for the function of hemoglobin- a protein in RBC thatPorphyrins are essential for the function of hemoglobin- a protein in RBC that links to porphyrin, binds iron and carries oxygen from lungslinks to porphyrin, binds iron and carries oxygen from lungs to different bodyto different body parts.parts. In the absence of certain enzymes, Porphyrin pathway is blocked during heme-In the absence of certain enzymes, Porphyrin pathway is blocked during heme- synthesis and Porphyrin & its precursors start building upsynthesis and Porphyrin & its precursors start building up in the body parts.in the body parts. The porphyrins that occur in first half of heme synthesis pathways areThe porphyrins that occur in first half of heme synthesis pathways are water-water- soluble & excreted through urine.soluble & excreted through urine. Porphyrias are either inherited (autosomal recessive/x-linked) or acquiredPorphyrias are either inherited (autosomal recessive/x-linked) or acquired (drug intoxication) mainly caused due to mutation in genes(drug intoxication) mainly caused due to mutation in genes which producewhich produce hemoglobin.hemoglobin. Heme production occurs in :Heme production occurs in : (1) Bone Marrow(1) Bone Marrow (2) Liver(2) Liver IntroductionIntroduction continued…continued…
- 4. Chart showing how absence of differentChart showing how absence of different enzymesenzymes causing differentcausing different porphyriaporphyria during heme-synthesis along with major symptoms & accumulated products.during heme-synthesis along with major symptoms & accumulated products.
- 5. Porphyrias can be classified in three different ways.Porphyrias can be classified in three different ways. (1)(1) On the basis of specific enzyme deficiency.On the basis of specific enzyme deficiency. (2)(2) On the basis of predominant symptoms seen or clinicalOn the basis of predominant symptoms seen or clinical manifestations.manifestations. (3)(3) On the basis where the excess precursors originate.On the basis where the excess precursors originate. Classification:Classification:
- 6. Classification on basis of Enzyme DeficiencyClassification on basis of Enzyme Deficiency
- 7. Acute Porphyria: Porphyria that causesAcute Porphyria: Porphyria that causes neurologic, mental & abdominal or gastricneurologic, mental & abdominal or gastric symptoms.symptoms. Cutaneous Porphyria: Porphyria thatCutaneous Porphyria: Porphyria that causes skin problemscauses skin problems when exposed towhen exposed to sunlight.sunlight. Classification on basis of Predominant SymptomsClassification on basis of Predominant Symptoms
- 8. NeuropsychiatricNeuropsychiatric:: 1.Acute intermittant porphyrias(AIP)1.Acute intermittant porphyrias(AIP) 2.ALA dehydratase porphyria(ADP)2.ALA dehydratase porphyria(ADP) Cutaneous(photosensitivity):Cutaneous(photosensitivity): 1.Congenital erythropoietic porphyria(CEP)1.Congenital erythropoietic porphyria(CEP) 2.Porphyria cutanea tarda(PCT)2.Porphyria cutanea tarda(PCT) 3.Erythropoietic porphyria(EPP)3.Erythropoietic porphyria(EPP) Mixed:Mixed: 1.Hereditary copro-porphyria(HCP)1.Hereditary copro-porphyria(HCP) 2.Variegate porphyria(VP)2.Variegate porphyria(VP) Classification based on predominant clinical manifestations:Classification based on predominant clinical manifestations:
- 9. Hepatic Porphyria:Hepatic Porphyria: (1) Acute Intermittent Porphyria (AIP)(1) Acute Intermittent Porphyria (AIP) (2) Porphyria Variegate (PV)(2) Porphyria Variegate (PV) (3) ADP(3) ADP (4) Hereditary Coproporphyria (HCP)(4) Hereditary Coproporphyria (HCP) Erythropoietic Porphyria:Erythropoietic Porphyria: (1) Protoporphyria.(1) Protoporphyria. (2) Uroporhyria(2) Uroporhyria Both:Both: (1) Porphyria Cutaneous Tarda (PCT)(1) Porphyria Cutaneous Tarda (PCT) Classification on basis where the excess precursorsClassification on basis where the excess precursors originatesoriginates
- 10. Seven major types of porhyria are nowSeven major types of porhyria are now recognized and may alsorecognized and may also be classified asbe classified as acuteacute andand non-acutenon-acute forms.forms.
- 11. The epidemiology is complicated and likely to be faulty becauseThe epidemiology is complicated and likely to be faulty because of its rarity.of its rarity. Its prevalence varies from country to country, as do the types ofIts prevalence varies from country to country, as do the types of porphyria.porphyria. An estimated geneAn estimated gene carriercarrier frequency for AIP in the generalfrequency for AIP in the general population of the USA is 1-2/10000, with clinical signs manifestpopulation of the USA is 1-2/10000, with clinical signs manifest in ~10%.in ~10%. Plumboporphyria has not been reported in thePlumboporphyria has not been reported in the UK.UK. Epidemiology:Epidemiology:
- 12. Porphyria is more common between adolescence andPorphyria is more common between adolescence and menopause.menopause. Four times as many symptomatic cases in women, with aFour times as many symptomatic cases in women, with a particular increase in premenstrual women.particular increase in premenstrual women. The prevalence of variegate porphyria among an AfrikaansThe prevalence of variegate porphyria among an Afrikaans population of South Africa is estimated at 1 inpopulation of South Africa is estimated at 1 in 250.250. It has been reported that acute porphyria is more common inIt has been reported that acute porphyria is more common in psychiatric patients of the general population.psychiatric patients of the general population. EpidemiologyEpidemiology continued…continued…
- 13. United StatesUnited States Estimates vary from 1-5 cases per 100,000 population.Estimates vary from 1-5 cases per 100,000 population. InternationalInternational Prevalence can be as high as 60-100 cases per 100,000Prevalence can be as high as 60-100 cases per 100,000 population inpopulation in northern Sweden.northern Sweden. SexSex In most series, AIP affects women more than men, with aIn most series, AIP affects women more than men, with a ratio of 1.5-2:1.ratio of 1.5-2:1. AgeAge Most patients become symptomatic at age 18-40 years.Most patients become symptomatic at age 18-40 years. Attacks occurring before puberty or after age 40 years are unusual unlessAttacks occurring before puberty or after age 40 years are unusual unless a major provocation, such as new use of phenobarbital or estrogens, hada major provocation, such as new use of phenobarbital or estrogens, had occurred.occurred. EpidemiologyEpidemiology continued…continued…
- 14. The enzyme deficiency in each of the 3 common acute disorders isThe enzyme deficiency in each of the 3 common acute disorders is only partial (~50%), the reduced enzyme activity being sufficient foronly partial (~50%), the reduced enzyme activity being sufficient for haem production under normal circumstances.haem production under normal circumstances. However, these deficiencies predispose people to the actions ofHowever, these deficiencies predispose people to the actions of precipitating agents, includingprecipitating agents, including drugs, endogenous steroids, cigarettedrugs, endogenous steroids, cigarette smoke,smoke, physiological stress during illness, psychological stress,physiological stress during illness, psychological stress, fasting and dieting – which all increase the liver haem demand, thusfasting and dieting – which all increase the liver haem demand, thus inducing ALA-S.inducing ALA-S. With increased ALA-S activity, haem synthetic intermediatesWith increased ALA-S activity, haem synthetic intermediates accumulate to the point where the partial enzymeaccumulate to the point where the partial enzyme deficienciesdeficiencies become limiting.become limiting. The intermediates then accumulate in the liver and begin to ‘spillThe intermediates then accumulate in the liver and begin to ‘spill over.’over.’ Pathogenesis:Pathogenesis:
- 16. PathogenesisPathogenesis continued…continued… The porphyrin precursors are neurotoxic to the ANS andThe porphyrin precursors are neurotoxic to the ANS and PNS.PNS. Histological investigation reveals oedema,Histological investigation reveals oedema, degenerating and irregular axons anddegenerating and irregular axons and damaged myelindamaged myelin sheaths.sheaths. The BBB does not protect the hypothalamus and the limbic area.The BBB does not protect the hypothalamus and the limbic area. Possible mechanisms of neurotoxicity:Possible mechanisms of neurotoxicity: ALA is structurally similar to GABA > disturbance ofALA is structurally similar to GABA > disturbance of neurochemicalneurochemical signalling.signalling. Porphyrin precursors may cause vascular injury > focalPorphyrin precursors may cause vascular injury > focal cerebralcerebral oedema.oedema. Cerebral vasospasm > multifocal ischemia.Cerebral vasospasm > multifocal ischemia.
- 17. Induction of the rate-limiting hepatic enzyme ALA synthase in heterozygotes withInduction of the rate-limiting hepatic enzyme ALA synthase in heterozygotes with half-normal HMB synthase activity.half-normal HMB synthase activity. AIP almost always latent before puberty –suggests adult levels ofAIP almost always latent before puberty –suggests adult levels of steroid hormonessteroid hormones are important for clinical expression.are important for clinical expression. Heterozygous forHeterozygous for HMBS mutations, causes for attacks of AIPHMBS mutations, causes for attacks of AIP prior toprior to puberty.puberty. Symptoms are more common in women, suggesting a role for estrogensSymptoms are more common in women, suggesting a role for estrogens oror progestins.progestins. Premenstrual attacks are probably due to endogenousPremenstrual attacks are probably due to endogenous progesterone.progesterone. Exacerbated by exogenous steroids, including OCP preparationsExacerbated by exogenous steroids, including OCP preparationscontainingcontaining progestinsprogestins Pregnancy, usuallywell tolerated, suggesting -beneficial metabolic changes -Pregnancy, usuallywell tolerated, suggesting -beneficial metabolic changes - ameliorates effects of high levels of progesterone.ameliorates effects of high levels of progesterone. Causative factors (Etiology):Causative factors (Etiology):
- 18. 1.Endogenous and exogenous steroids1.Endogenous and exogenous steroids 2.Porphyrinogenic drugs2.Porphyrinogenic drugs 3.Alcohol ingestion3.Alcohol ingestion 4.Low-calorie diets, usually instituted for weight loss4.Low-calorie diets, usually instituted for weight loss 5.Starvation5.Starvation 6.Infection6.Infection 7.Drugs: Barbituates, Sulphonamides7.Drugs: Barbituates, Sulphonamides Attacks can be prevented by avoiding known precipitating factors.Attacks can be prevented by avoiding known precipitating factors. Common precipitating factors :Common precipitating factors :
- 19. Abdominal painAbdominal pain,, peripheral neuropathyperipheral neuropathy and changes in theand changes in the mental statemental state are said to be the classic triad of an acute attack.are said to be the classic triad of an acute attack. An attack begins with behavioural changes: anxiety,An attack begins with behavioural changes: anxiety, restlessnessrestlessness and insomnia.and insomnia. The abdominal pain is severe and is followed by constipation andThe abdominal pain is severe and is followed by constipation and vomiting. Pain in the back and limbsvomiting. Pain in the back and limbs may also occur.may also occur. Increased BP and tachycardia reflect increased SNS activity.Increased BP and tachycardia reflect increased SNS activity. Clinical manifestations:Clinical manifestations:
- 20. The pain resolves within 7 days.The pain resolves within 7 days. However, if a precipitating agent (see later) is inadvertentlyHowever, if a precipitating agent (see later) is inadvertently given, a progressive neuropathy with muscle weakness,given, a progressive neuropathy with muscle weakness, decreased reflexes and ‘socks and gloves’ sensory loss maydecreased reflexes and ‘socks and gloves’ sensory loss may become apparent and can lead tobecome apparent and can lead to respiratoryrespiratory paralysis.paralysis. Clinical manifestationsClinical manifestations continued…continued…
- 21. As the autonomic neuropathy progresses,As the autonomic neuropathy progresses, arrhythmias emergearrhythmias emerge and may precede a cardiacand may precede a cardiac arrest.arrest. Muscle weakness may progress to a quadriparesis and respiratoryMuscle weakness may progress to a quadriparesis and respiratory muscle paralysis, mimickingmuscle paralysis, mimicking Guillain-Barré syndrome.Guillain-Barré syndrome. Cardiac arrest and pneumonia associatedCardiac arrest and pneumonia associated with prolonged artificial ventilation arewith prolonged artificial ventilation are common causes of death at this stage.common causes of death at this stage. Clinical manifestationsClinical manifestations continued…continued…
- 22. Hyponatraemia often occurs with attacks of acute porphyria.Hyponatraemia often occurs with attacks of acute porphyria. (Na+ RR: 135-(Na+ RR: 135-145mmol/L)145mmol/L) Although not fully understood, damage to the supraoptic nucleiAlthough not fully understood, damage to the supraoptic nuclei of the hypothalamus leading to SIADH has been implicated.of the hypothalamus leading to SIADH has been implicated. Clinical manifestationsClinical manifestations continued…continued…
- 23. Skin lesions accompany acute attacks in 1/2 of people withSkin lesions accompany acute attacks in 1/2 of people with variegate porphyria and 1/3 of those with hereditaryvariegate porphyria and 1/3 of those with hereditary coproporphyria.coproporphyria. Clinical manifestationsClinical manifestations continued…continued…
- 24. Anxiety, depression, insomnia and restlessness are often presentAnxiety, depression, insomnia and restlessness are often present and may persist between attacks.and may persist between attacks. In one case study, attacks of AIP presented with impulsiveIn one case study, attacks of AIP presented with impulsive behaviour, low mood and suicide attempts.behaviour, low mood and suicide attempts. Another has described the schizophrenic symptoms of socialAnother has described the schizophrenic symptoms of social withdrawal, persecutory delusions andwithdrawal, persecutory delusions and auditory hallucinations.auditory hallucinations. Conversion disorder, somatisation disorder and CFS have alsoConversion disorder, somatisation disorder and CFS have also been described.been described. Psychiatric manifestations:Psychiatric manifestations:
- 25. During attacks, the 4 acute porphyrias areDuring attacks, the 4 acute porphyrias are indistinguishableindistinguishable clinically.clinically. Patients may experience different symptoms during repeatPatients may experience different symptoms during repeat attacks.attacks. As the attacks mimic other medical and psychiatric disorders, theAs the attacks mimic other medical and psychiatric disorders, the diagnosis ofdiagnosis of porphyria is difficult.porphyria is difficult. In a patient with abdominal pain the features of rapid onsetIn a patient with abdominal pain the features of rapid onset hypertension, low Na, proximal muscle weakness, history of lowhypertension, low Na, proximal muscle weakness, history of low carbohydrate diets and recent use of Porphyrinogenic drugscarbohydrate diets and recent use of Porphyrinogenic drugs increases the likelihood of an acute porphyria.increases the likelihood of an acute porphyria. Clinical manifestationsClinical manifestations summary:summary:
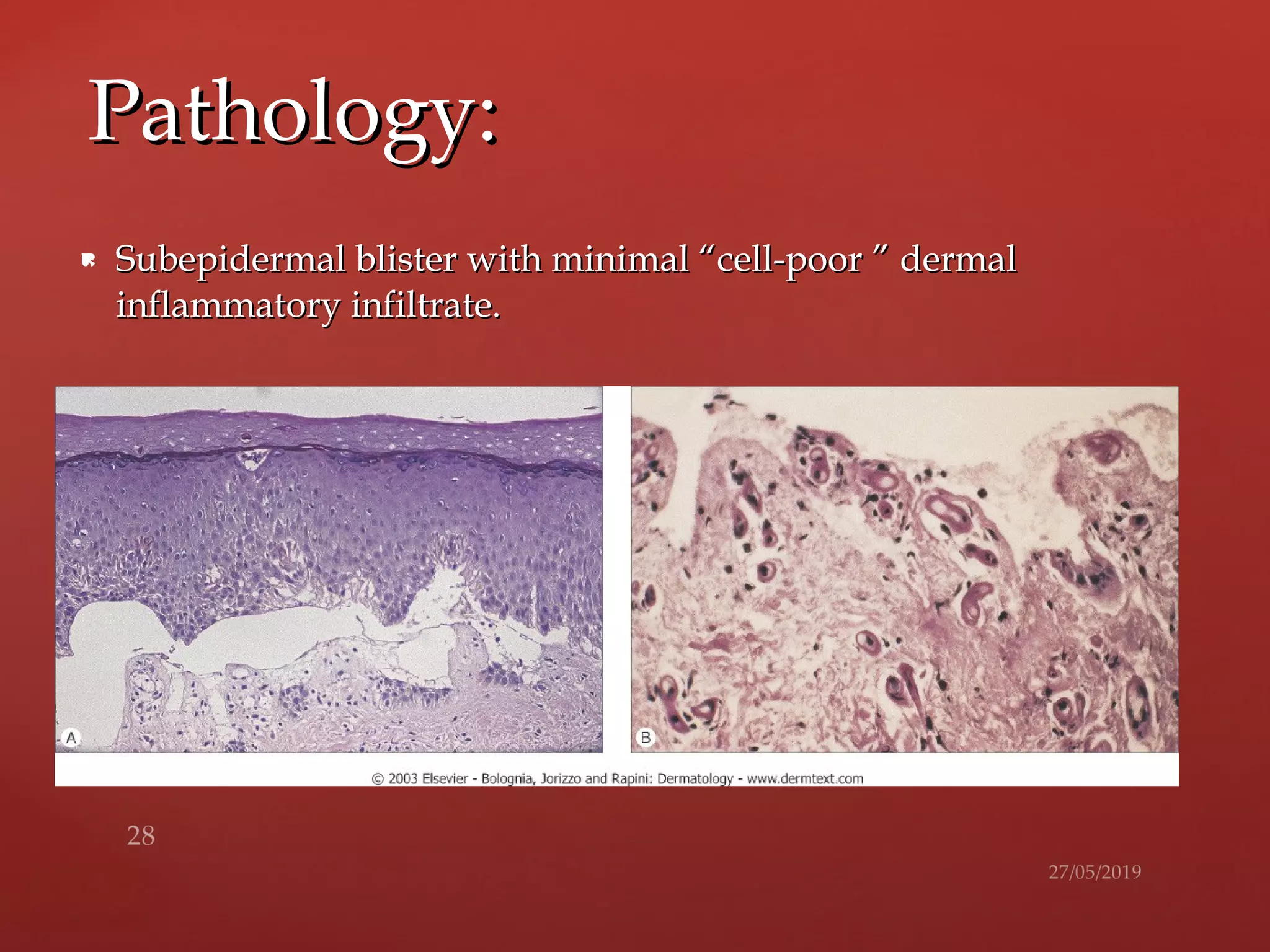
- 28. Subepidermal blister with minimal “cell-poor ” dermalSubepidermal blister with minimal “cell-poor ” dermal inflammatory infiltrate.inflammatory infiltrate. Pathology:Pathology:
- 29. Sudden death-results from sympathetic overactivity andSudden death-results from sympathetic overactivity and cardiaccardiac arrhythmia.arrhythmia. CirrhosisCirrhosis Renal FailureRenal Failure Neurological SequelaeNeurological Sequelae Hepatic Cellular CarcinomaHepatic Cellular Carcinoma Chronic depression and suicideChronic depression and suicide Long Term ComplicationsLong Term Complications & causes of death:& causes of death:
- 31. Shafer’s textbook of Oral Pathology-Shafer, Hine, LevyShafer’s textbook of Oral Pathology-Shafer, Hine, Levy Oral & Maxillofacial Pathology-Neville, Damm, Allen,Oral & Maxillofacial Pathology-Neville, Damm, Allen, BouqotBouqot Pathologic Basis of Disease- Robbins & Cotran.Pathologic Basis of Disease- Robbins & Cotran. Essential Pathology for Dental Students-Harsh Mohan.Essential Pathology for Dental Students-Harsh Mohan. WikipediaWikipedia emedicine.medscape.comemedicine.medscape.com Porphyriafoundation.comPorphyriafoundation.com MSD Manual Professional EditionMSD Manual Professional Edition Main References:Main References: