The ankle joint (or talocrural joint) is a synovial joint located in the lower limb. It is formed by the bones of the leg (tibia and fibula) and the foot (talus).
Functionally, it is a hinge type joint, permitting dorsiflexion and plantarflexion of the foot.
In this article, we shall look at the anatomy of the ankle joint; its articulating surfaces, ligaments, movements, and clinical correlations.
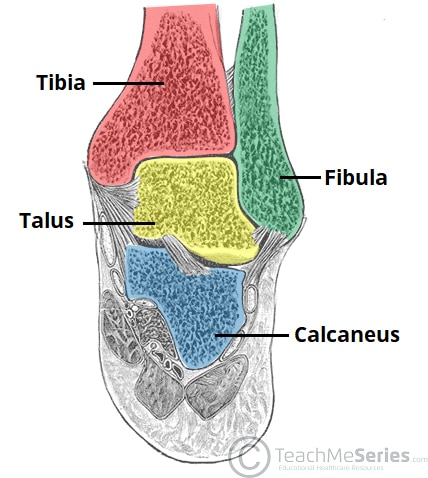
Fig 1
The bones of the ankle joint; tibia, fibula and talus. Note that the calcaneous is not considered part of the ankle joint.
Premium Feature
3D Model
Articulating Surfaces
The ankle joint is formed by three bones; the tibia and fibula of the leg, and the talus of the foot:
The tibia and fibula are bound together by strong tibiofibular ligaments. Together, they form a bracket shaped socket, covered in hyaline cartilage. This socket is known as a mortise.
The body of the talus fits snugly into the mortise formed by the bones of the leg. The articulating part of the talus is wedge shaped – it is broad anteriorly, and narrow posteriorly:
- Dorsiflexion – the anterior part of the talus is held in the mortise, and the joint is more stable.
- Plantarflexion – the posterior part of the talus is held in the mortise, and the joint is less stable.
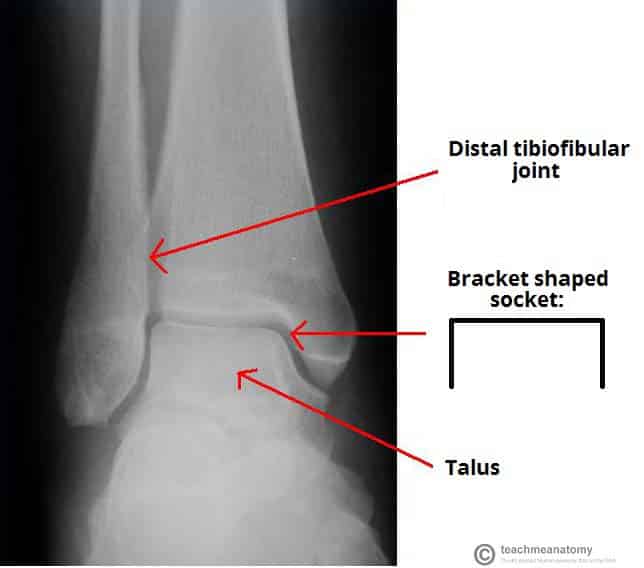
Fig 2
X-ray of a normal ankle joint. Note the bracket shaped socket formed by the tibia and fibula.

Fig 3
The talus. It is broad anteriorly, which strengthens the joint during dorsiflexion.
Ligaments
There are two main sets of ligaments, which originate from each malleolus.
Medial Ligament
The medial ligament (or deltoid ligament) is attached to the medial malleolus (a bony prominence projecting from the medial aspect of the distal tibia).
It consists of four ligaments, which fan out from the malleolus, attaching to the talus, calcaneus and navicular bones. The primary action of the medial ligament is to resist over-eversion of the foot.
Lateral Ligament
The lateral ligament originates from the lateral malleolus (a bony prominence projecting from the lateral aspect of the distal fibula).
It resists over-inversion of the foot, and is comprised of three distinct and separate ligaments:
- Anterior talofibular – spans between the lateral malleolus and lateral aspect of the talus.
- Posterior talofibular – spans between the lateral malleolus and the posterior aspect of the talus.
- Calcaneofibular – spans between the lateral malleolus and the calcaneus.
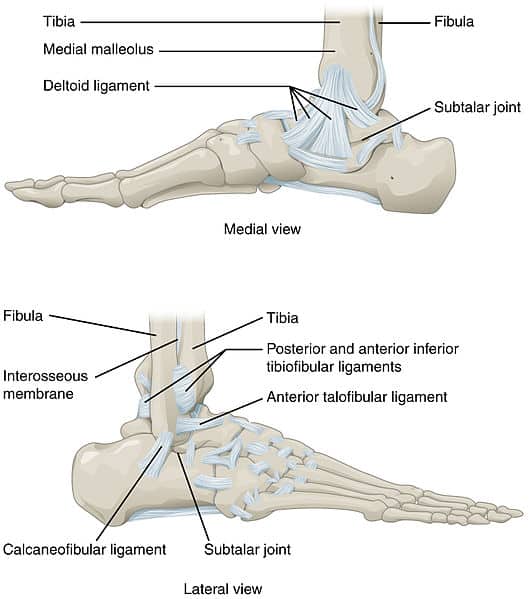
Fig 4
Ligaments of the ankle joint.
Clinical Relevance
The Ankle ‘Ring’
The ankle joint and associated ligaments can be visualised as a ring in the coronal plane:
- The upper part of the ring is formed by the articular surfaces of the tibia and fibula.
- The lower part of the ring is formed by the subtalar joint (between the talus and the calcaneus).
- The sides of the ring are formed by the medial and lateral ligaments.
A ring, when broken, usually breaks in two places (the best way of illustrating this is with a polo mint – it is very difficult to break one side without breaking the other).
When dealing with an injury to the ankle joint, a clinician must bear this in mind. For example, a fracture of the ankle joint may occur in association with ligament damage (which would not be apparent on x-ray).
Movements and Muscles Involved
The ankle joint is a hinge type joint, with movement permitted in one plane.
Thus, plantarflexion and dorsiflexion are the main movements that occur at the ankle joint. Eversion and inversion are produced at the other joints of the foot, such as the subtalar joint.
- Plantarflexion – produced by the muscles in the posterior compartment of the leg (gastrocnemius, soleus, plantaris and posterior tibialis).
- Dorsiflexion – produced by the muscles in the anterior compartment of the leg (tibialis anterior, extensor hallucis longus and extensor digitorum longus).
Neurovascular Supply
The arterial supply to the ankle joint is derived from the malleolar branches of the anterior tibial, posterior tibial and fibular arteries.
Innervation is provided by tibial, superficial fibular and deep fibular nerves.
Clinical Relevance
<strong>Ankle Sprain</strong>
An ankle sprain refers to partial or complete tears in the ligaments of the ankle joint. It usually occurs via excessive inversion to a plantarflexed and weight-bearing foot.
The lateral ligament is more likely to be damaged for two main reasons:
- The lateral ligament is weaker than the medial ligament.
- The lateral ligament resists inversion.
The anterior talofibular ligament is the lateral ligament most at risk of irreversible damage.
Clinical Relevance
<strong>Pott’s Fracture-Dislocation</strong>
A Pott’s fracture is a term used to describe a bimalleolar (medial and lateral malleoli) or trimalleolar (medial and lateral malleoli, and distal tibia) fracture.
This type of injury is produced by forced eversion of the foot. It occurs in a series of stages:
- Forced eversion pulls on the medial ligaments, producing an avulsion fracture of the medial malleolus.
- The talus moves laterally, breaking off the lateral malleolus.
- The tibia is then forced anteriorly, shearing off the distal and posterior part against the talus.

Fig 5
Bimalleolar fracture of the ankle. 1 – Fibula, 2 – Tibia.