




The hip is a ball-in-socket joint. It is comprised of the large, upper thigh bone (femur) where it inserts into the socket of the pelvis (acetabulum). The hip joint is very stable as it is a relatively deep socket, therefore it is hard to dislocate the hip joint when sudden, external forces are applied.
This is in stark contrast to the shoulder joint that is also a ball-in-socket. The shoulder joint is quite unstable since the shoulder socket is a shallow joint and it is much easier to dislocate when a sudden external force is applied.
A cartilaginous ring surrounds the rim of the hip socket, which also helps to improve the stability of the joint. This cartilaginous ring is called the labrum.


As mentioned previously, the causes of hip pain symptoms can originate at several different structures that are found both in and around the hip joint.
Let’s explore these potential medical conditions more so that you can get a good handle on the potential causes of your hip pain as well as what treatment options are available for each.
Hip osteoarthritis, which is also known as simply hip OA or hip arthritis, is a natural degenerative process within the joint. Osteoarthritis and rheumatoid arthritis are among the most common causes of hip pain, especially in older adults.
As we age, the cartilage at the ends of our bones, which cushions our joints, gradually wears down as they are exposed to repetitive stress and compression. I like to describe it as similar to the tread on a tire. Over time, the wear and tear on the tire will slowly erode down the tread.
In response to these high-stress areas, our bodies respond by building up excessive bone as a means of extra protection. In the hip joint, osteoarthritis is most commonly found on both the ball and socket sides of the joint. On an x-ray, I think it appears as though the femoral head closely resembles a head of cauliflower with a bunch of bony “nubs” scattered about.


Pain symptoms of hip osteoarthritis are typically described as a constant dull, toothache-like pain that refers to the outside of the hip and also toward the groin. Additionally, the hip joint may grind, pop, or click when moved. The symptoms usually worsen gradually over time as this is a progressive degeneration of the joint.
Many of my patients don’t initially suspect hip osteoarthritis because they feel the pain symptoms coming from the outside or outer backside of the hip. However, after further assessment, it is determined that the pain is being referred from the joint to these areas.


The first line of defense for treating hip osteoarthritis is participating in physical therapy. Physical therapy exercises will attempt to restore joint mobility and will improve joint stability by strengthening supporting musculature.
Additionally, research has proven that losing weight, even small amounts of up to 10 lbs, can have immediate impacts on reducing hip osteoarthritic pain as it reduces the compression across the joint.
Ultimately, if the osteoarthritis is too advanced and the daily functional tolerance of the individual is greatly impacted, a total hip arthroplasty (hip replacement) procedure will likely be recommended. Luckily, these patients recover exceptionally well these days. I see several of these patients weekly in my clinic.
On average, these patients will be back to daily functioning capacity (i.e. daily walks, kneeling, etc.) around 3-4 months post-operatively and they can progress to higher-level functional activities (i.e. hiking, etc.) around 6 months.


Avascular necrosis, also known as osteonecrosis, occurs when the blood flow decreases within the bones. When this occurs in the femur, the cartilage at the head of the femur slowly degrades and dies.
Avascular Necrosis be caused by several reasons including:
Fracture
Dislocation
Long-term use of steroids (i.e. Prednisone, Dexamethasone)
Other chronic medical conditions
Hip pain caused by avascular necrosis will be similar to osteoarthritis where the symptoms include a dull, toothache-like pain that can be referred to the groin, outer hip, and buttocks.


An X-ray, magnetic resonance imaging (MRI), and a bone scan of your hip will likely be ordered to better understand the severity of this condition. The results will be used to develop a treatment plan for you. Nonsteroidal anti-inflammatory medications may be recommended by your doctor to help manage the pain symptoms.
Physical therapy exercises and stretches can help to maintain the optimal range of motion of the hip joint while improving the strength in the muscles that support the joint.
Depending on the severity of the condition, surgical options for the treatment of Avascular Necrosis may include:
Femoral Head Decompression
Bone Transplant
Total Hip Arthroplasty (Replacement)
Hip bursitis (also known as trochanteric bursitis) is simply the inflammation of the hip bursa. A bursa is a fluid-filled sac that is meant to pad the space between soft tissue (i.e. muscles, tendons) and bones. This padding will prevent irritation and inflammation from occurring as, without the bursa, the soft tissue may rub against the bone and possibly lead to fraying or tearing of the tissue.
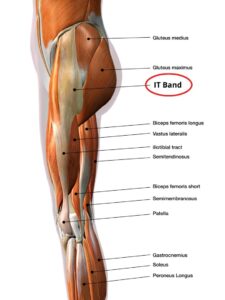
The hip bursa (medical name: greater trochanteric bursa) is located on the outside of the hip near the hip bone (greater trochanter) that protrudes out from the side of your hip. It lies directly underneath the Iliotibial Band (IT Band) and pads the space between the IT Band and the hip bone.


Hip bursitis is more frequently seen in older, adult females. However, I have treated a handful of older men with hip bursitis too, so they too can get it.
Women tend to develop bursitis more often because, genetically, they tend to skeletally develop with wider hips when compared to males. This increased width allows for the passage of a child during birth. Unfortunately, the extra width also sets them up with a bio-mechanical disadvantage because the hip muscles are set up at a greater angle to their insertion points on the hip bones resulting in greater weakness in the muscles.
Ultimately, with more weakness in the hips comes increased tightness in the muscles and fascia in the outer hip. The tightness begins to slowly increase over time. The tightness begins to compress the bursa underneath against the hip bone. This process could take many months or even years. Usually, the person does not even notice the gradual change.
Eventually, the compression is too much for the bursa and it starts to become inflamed. Pain is now present. These hip pain symptoms are typically described as a constant, dull ache that refers from the hip down the outside of the thigh towards the knee. The pain would increase with sustained standing and walking activities. Lying on the painful side would increase the pain.
Physical therapy is again the first line of defense for hip bursitis. Since this is a compressive disorder, there are some critical precautions that an individual should be educated on so that continual aggravation of the hip pain symptoms does not continue.
If you have not yet read my full article on hip bursitis exercises, head on over and check it out. It will describe all of the need-to-know information on this topic.
If the pain is severe, or if the pain is not drastically improving with physical therapy exercises, the individual would likely benefit from a corticosteroid injection into the bursa. The injection will have an immediate effect of decreasing the pain and reducing the inflammation.
However, don’t be fooled that you should stop doing your physical therapy exercises just because you get an injection. Just because the pain may be reduced, the initial cause of the irritation has not been addressed, so continue to follow the guidance in my hip bursitis exercises article to prevent future setbacks.

- TWO 3.5oz/100g TUBES OF VOLTAREN PAIN GEL
- POWERFUL TOPICAL PAIN RELIEF
- NONSTEROIDAL ANTI-INFLAMMATORY
- NUMBER 1 DOCTOR RECOMMENDED TOPICAL PAIN RELIEF
Diclofenac sodium (brand name: Voltaren Gel) is an over-the-counter anti-inflammatory topical gel that may also be considered for use with hip bursitis. You can find it in most pharmacies. This gel will be rubbed over the painful area several times a day. It soaks through the skin and works on the irritated soft tissue underneath. Remember to talk to your doctor or physical therapist before using any topical creams to ensure that it is safe for you to try.


The Gluteus Medius muscle is a hip abductor muscle that is located at the outside of the pelvis/hip. The muscle helps to stabilize the pelvis when you are standing on a single leg (think when walking as the opposite leg swings forward). Sometimes this muscle can tear near its insertion into the bone, which is located at the outer hip bone (greater trochanter).


Similar to hip bursitis, a Gluteus Medius tear will cause outer hip pain symptoms. These symptoms often include a constant dull, ache-type pain with random episodes of sharp, stabbing pain that worsens with walking, standing, and other weight-bearing activities.
A Gluteus Medius tear and hip bursitis are often difficult to differentiate because the location of the symptoms is so similar. Oftentimes, the muscle tear is not diagnosed until a bout of physical therapy has been attempted without successful improvement in hip pain.
Since this muscle helps to stabilize the pelvis, a clinical test to assess if it’s torn is to have the patient lie on his/her non-painful side and attempt to raise the painful leg (knee straight) towards the ceiling. If there is a significant tear in the muscle, the leg will not be able to raise up successfully. This is referred to as a Hip Lag Sign.


Physical therapy exercises should be performed for 4-6 weeks to assess if the patient’s hip pain symptoms can improve with conservative care.
However, if the hip pain and strength do not improve with therapeutic exercise, the muscle tear will likely need to be surgically repaired.
Unfortunately, the post-operative hip precautions are very strict at the patient will not be allowed to place any weight on the surgical leg until 6 weeks post-op. This is to protect the repair while it is healing. During this time, the patient will be required to ambulate on just one leg while using either a walker or crutches for assistance.
Hip impingement is a very common condition that I see in my clinic weekly. Medically it is known as femoroacetabular impingement or FAI as it occurs in the joint space between the femur (ball) and the acetabulum (socket).
Impingement will typically cause people hip pain during and after bouts of higher intensity (running, squatting, jumping, crouching, etc.) As you may have guessed then that it occurs more often in younger adolescents and adults who are active.
There are 3 types of hip impingement.
Cam
Pincer
Combined
If you would like to read in more detail on the types of impingement, you can check out this great article from the American Academy of Orthopaedic Surgeons.
Without getting into too much detail for this article though, all three of these types of impingement are caused by excessive bone growth within the joint. Due to this excessive bone, the joint no longer has the ability to go through its full range of motion without coming into contact with the other bones in the joint space. Over time this repetitive contact will likely lead to other issues such as a labral tear.
The hip pain symptoms that it produces are usually a sharp pinching or locking sensation in the hip joint. These symptoms occur when moving the hip or bearing weight through the leg when walking.
Over-the-counter medications such as nonsteroidal anti-inflammatories may be recommended by your doctor to help decrease the inflammation and pain symptoms in the hip. These medications should be combined with rest from any possible aggravating activities to allow the hip symptoms to dissipate.
Physical therapy exercises and stretches can help to restore joint mobility and strengthen the muscles that support the joint.
If you continue to experience sharp, stabbing pains in your hip after a trial for 4-6 weeks of physical therapy, you will likely be referred for an MRI by an orthopedic surgeon.
The surgeon will assess the severity of the cam or pincher deformity and make a recommendation that may include:
Corticosteroid Injection
Labral Debridement - Surgical removal and/or shaving down of any labral tear that may be present
Labral Repair
Femoroplasty
Surgical removal of the cam or pincher deformity
Fractures of the femur usually require blunt force trauma such as a fall or involvement in a motor vehicle accident. Fractures can also be caused by certain bone cancers or a gradual weakening of the bones (osteoporosis), which is more common in older individuals.
Pain symptoms caused by a hip fracture include sudden, severe pain in the hip/leg that is worsened when putting body weight through the leg. The symptoms are usually severe enough that it prevents the person from being able to walk or stand normally.


This condition is considered a medical emergency. Call 911 or take the individual immediately to the nearest emergency room. Depending on the severity and the amount of bone displacement at the fracture site, surgery may or may not be required.
Physical therapy will be necessary to help restore the function of the hip once the doctor clears the individual for participation in therapy.
External Snapping Hip Syndrome is an overuse injury. It occurs when the Iliotibial band (IT band) becomes excessively tight along the outer leg/hip. The increased tightness causes the IT band to “snap or pop” over the outer hip bone (greater trochanter), rather than smoothly passing over it as the hip goes from a flexed position to an extended position (think walking, running, etc).
The snapping and popping can both be audible and palpable in nature depending on the severity of tightness in the IT band. If not treated appropriately, the repetitive snapping over the bone can lead to IT band Syndrome (pain and inflammation in the IT band) or Hip Bursitis.


Hip pain symptoms from external snapping hip syndrome can include:
Dull, ache-type pain along the outer hip running down the outside of the thigh towards the knee
Popping or snapping of the IT band around the outer hip bone
External Snapping Hip Syndrome symptoms will worsen with activity and are better with rest.
Rest from aggravating activities should begin immediately. During this rest period, perform physical therapy exercises to strengthen the glute complex and stretch out the hip muscles. IT band myofascial release (using a foam roller or massage roller stick) will help to reduce the tightness in the IT band allowing it to pass smoothly over the outer hip bone, rather than snapping over it.
Internal Snapping Hip Syndrome, also known as dancer’s hip, is an overuse injury that is caused by excessive tightness in the hip flexor muscles. This is most commonly seen in active individuals such as athletes who participate in sports that require strong hip flexor activation (runners, jumpers, dancers).
Internal Snapping Hip Syndrome is most commonly caused by the iliopsoas muscle group. The iliacus and psoas hip flexor muscles meet together to form the iliopsoas as they pass over the top of the pubic crest bone in the pelvis. When the iliopsoas becomes excessively tight, it can begin to “snap or pop” over the bone when the hip goes from a flexed position to an extended position.


If this condition is not treated appropriately, iliopsoas tendinitis (inflammation of the iliopsoas) can develop from the repetitive irritation of the muscle snapping down over the bone. These symptoms worsen with activity and are better with rest.
Since Internal Snapping Hip Syndrome is an overuse injury, rest from aggravating activities and physical therapy stretches should be initiated immediately. The stretches should focus on reducing the tightness in the hip flexor muscle groups. Strengthening of the hip extensors (glutes) can help to balance out the strength of the hip flexors.
If 4-6 weeks of physical therapy does not help to reduce these hip pain symptoms, a consultation with an orthopedic surgeon can be helpful. There is a procedure called an endoscopic iliopsoas release surgery that can be performed in severe cases. Our bodies have secondary hip flexor muscles, so it is possible to live a normal life without the iliopsoas intact.
IT Band Syndrome is an overuse injury that typically relates very closely to Hip Bursitis and External Snapping Hip Syndrome. All of these conditions are caused by excessive tightness in the IT Band as it passes over the outer hip bone (greater trochanter).

The IT Band helps to support the pelvis. It can become increasingly tight from repetitive hip flexion activities (running, stair ambulation, hiking, etc), sudden increases in weight gain, and excessive weakness in the hip abductor muscles.
As the tightness in the IT Band increases, it begins to rub on the outer hip bone as it passes over the top of it when the hip moves from a hip flexed to a hip extended position.
Hip pain symptoms for this syndrome will include a dull, ache coming from the outer hip. Additionally, there will be tenderness to palpation along the outside of the hip running down the IT Band along the outer thigh. These symptoms worsen with activity and are better with rest.
The first intervention should be temporary rest from aggravating activities to allow for a decrease in pain and inflammation within the IT Band.
Physical therapy exercises should be performed with the goal to decrease the tightness and irritation of the hip musculature including the IT Band. Since the IT Band is not a muscle, you cannot stretch it with a traditional muscle stretch. Rather, use a foam roller or a massage roller stick to perform myofascial release to reduce the stiffness in it. You can read about exactly how to do this in my “Best Exercises for Knee Pain Relief” article.
- TWO 3.5oz/100g TUBES OF VOLTAREN PAIN GEL
- POWERFUL TOPICAL PAIN RELIEF
- NONSTEROIDAL ANTI-INFLAMMATORY
- NUMBER 1 DOCTOR RECOMMENDED TOPICAL PAIN RELIEF
Diclofenac sodium (brand name: Voltaren Gel) is an over-the-counter anti-inflammatory topical gel that may also be considered for use with IT Band Syndrome. This gel will be rubbed over the painful area several times a day. It soaks through the skin and works on decreasing the inflammation in the irritated soft tissue underneath. Be sure to check with your doctor before using any medications to make sure it is safe for you to use.
In severe cases, a corticosteroid injection to the area of irritation may be recommended to help promote a reduction in inflammation and improve the individual’s tolerance to physical therapy exercises.
A hip labral tear involves the labrum, which is a cartilaginous ring that helps to deepen and stabilize the hip socket. Think of it like a rubber seal surrounding the socket. Tearing of this tissue is most commonly seen in adolescents and younger adults. The labrum typically tears with rotation, high impacts (jumping), and heavy loading (lifting).
Symptoms from a labral tear can include a constant dull, ache in the buttocks, groin, or outer thigh that can be sharp, stabbing pain when performing weight-bearing activities. These symptoms worsen with activity and are better with rest.
A corticosteroid injection may be recommended to help promote the reduction of pain and inflammation in the hip joint. In cases with severe hip pain, it can help to improve an individual’s tolerance to physical therapy.
Physical therapy exercises should be performed to promote improved hip mobility, flexibility, and stability.
If no improvement with physical therapy is seen after 4-6 weeks of daily performance, an MRI will likely be recommended to assess the severity and location of the tear. A consultation with an orthopedic surgeon will be beneficial to understand the surgical options for each case, which may include:
Labral Debridement (removal/shaving down of any labral tear that may be present)
Labral Repair
A sports hernia, also known as athletic pubalgia, is a soft tissue injury that occurs to the muscles, tendons, or ligaments in the groin area. These injuries tend to occur most often in sports that require sudden changes in direction or twisting motions.
The structures that are most commonly injured are located where the tendons of the oblique muscles and hip adductor muscles insert into the pubic bone. The tendons can become stretched (strained) or even torn.


The hip pain symptoms from a sports hernia are located closer to the groin area and are typically described as a constant ache-type pain with sharp, stabbing pain when the muscles are contracted against resistance. The symptoms typically are relieved with rest. There can be a visible bulge similar to a traditional inguinal hernia, but not always.
The first intervention for a sports hernia is rest. This will allow for a decrease in tissue inflammation and irritation resulting in decreased pain symptoms.
Physical therapy exercises should be started soon after to restore flexibility and strength of the hip and groin muscles.
After 8 weeks of physical therapy with no or little improvements, a consultation with an orthopedic surgeon should be considered.
There are a few surgical interventions that are available:
Surgical Repair of the Torn Tissue
Neurectomy
Cutting of the nerve in the groin region to permanently decrease the pain symptoms
Adductor tenotomy
Cutting of the involved adductor muscle tendon where it attaches to the bone as it will heal back with less tension through it, resulting in decreased pain symptoms






