Chiropractic Hand And Wrist Physical Exam
Reading time: 6 minutes
Hand and wrist conditions comprise a significant portion of all MSK presentations, including up to 25% of all sports injuries. (1,2) Fortunately, evidence-based chiropractors are very well-suited to manage many of those patients successfully… IF we nail the diagnosis. This week’s blog and video will cover the evaluation essentials, including a straightforward wrist and hand exam tutorial to help Up your A-game!
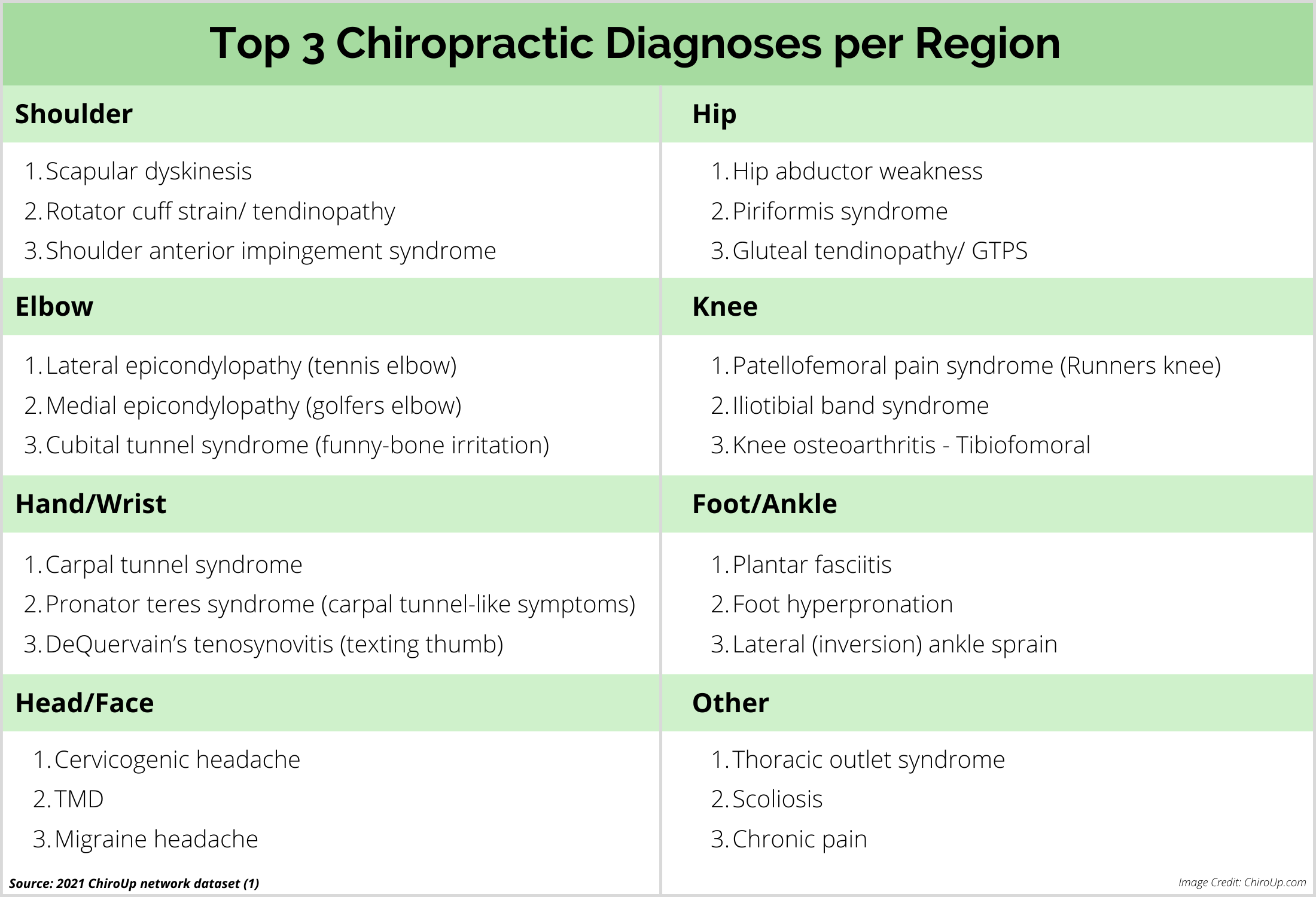
According to the 2021 ChiroUp Network Dataset Analysis of 631,970 clinical diagnoses collected from our 2,200 evidence-based chiropractic providers, the top three most common hand and wrist pain diagnoses in chiropractic offices were:
Carpal tunnel syndrome
Pronator teres syndrome
DeQuervain’s tenosynovitis
While it’s no surprise that overuse neuropathies and tendinopathies top the list, providers must consider several other potential wrist and hand pain diagnoses affecting the numerous bones, joints, cartilage, ligaments, tendons, muscles, and nerves:
Trauma
Fracture
Dislocation
Muscle/ tendon strain
Ligament sprain
Triangular fibrocartilage complex (TFCC)
Microtrauma
Joint dysfunction (hypo- or hyper-mobility)
Osteoarthritis
Ganglion cyst
Tendinopathy:
De Quervain's
Trigger finger
Neuropathy:
Carpal tunnel
Pronator teres
Radial tunnel
Cubital tunnel
Disease
Inflammatory arthropathy
Less common threatening presentations:
Avascular necrosis
Infection
Neoplasm
Orthopedic experts estimate that the patient history highlights a specific diagnosis in approximately 70% of hand and wrist presentations. (3) Key wrist and hand exam history questions include:
Trauma history - a fall on an extended hand is a common mechanism for sprain/strains, fractures, and dislocations.
Occupation and activities (aka Microtrauma history) - overuse disorders, particularly osteoarthritis, tendinopathies, and neuropathies, are usually tied to a predictable history of repetitive microtrauma. And don’t forget to ask about handedness- cumulative use disorders, including carpal tunnel syndrome, are more common in the dominant hand. (4,5)
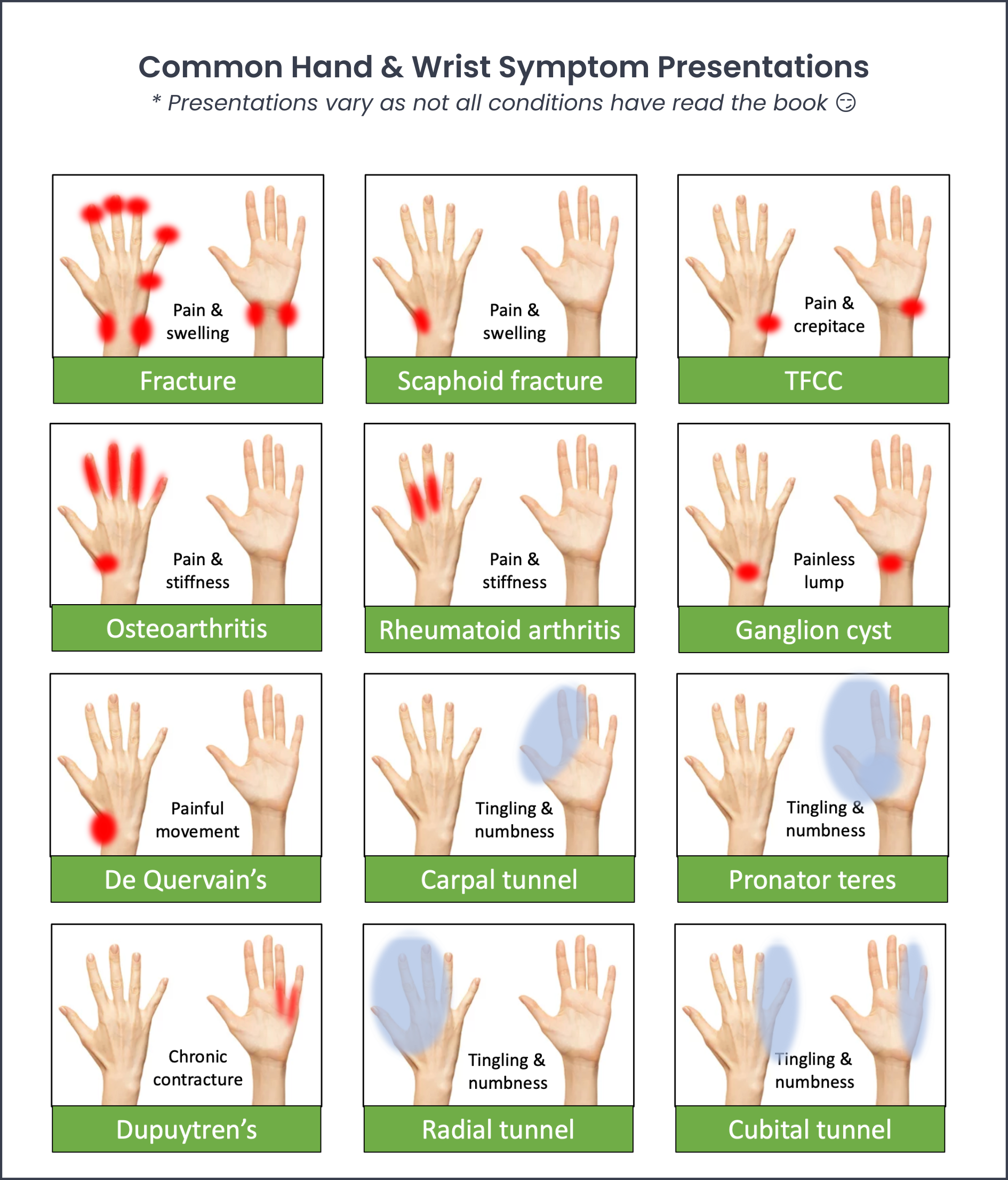
Symptom location and character - predictable patterns of pain, stiffness, and numbness or tingling each suggest a potentially different structural etiology. Check out this hand and wrist symptoms chart for a quick synopsis.
In addition to the standard OPPQRST inquiry, other essentials questions include:
Morning stiffness - hand osteoarthritis patients complain about being rusty for the first half hour; however, stiffness that lasts beyond 30 minutes could suggest an inflammatory arthropathy like rheumatoid, psoriatic, lupus, or gout.
Health history - conditions including psoriasis, thyroid disease, renal disease, alcoholism, vitamin D deficiency, diabetes, osteoporosis, and pregnancy can be a predisposing factor or trigger for various hand and wrist complaints. And don’t skip the family history to uncover a genetic predisposition for inflammatory arthropathies.
The essential components of a chiropractic wrist and hand physical exam include:
Inspection - swelling, deformity, discoloration, skin or nail changes
Range of motion - active, passive, resisted movements
General palpation - tenderness, swelling, warmth, muscle wasting, distal pulse intensity
Joint palpation - squeeze, stability testing, motion palpation
Orthopedic assessment - specific to the differential diagnoses
Neurodynamic testing - median, radial, ulnar nerves
Cervical evaluation - don’t forget an estimated 38% of hand and wrist problems arise from an asymptomatic spine (6)
Watch this tutorial on performing a straightforward orthopedic wrist and hand exam.
While most hand and wrist presentations are not overly concerning, providers should be vigilant for a few common hand and wrist differential diagnoses that pose significantly more sinister threats—each of the following warrants specialist consultation.
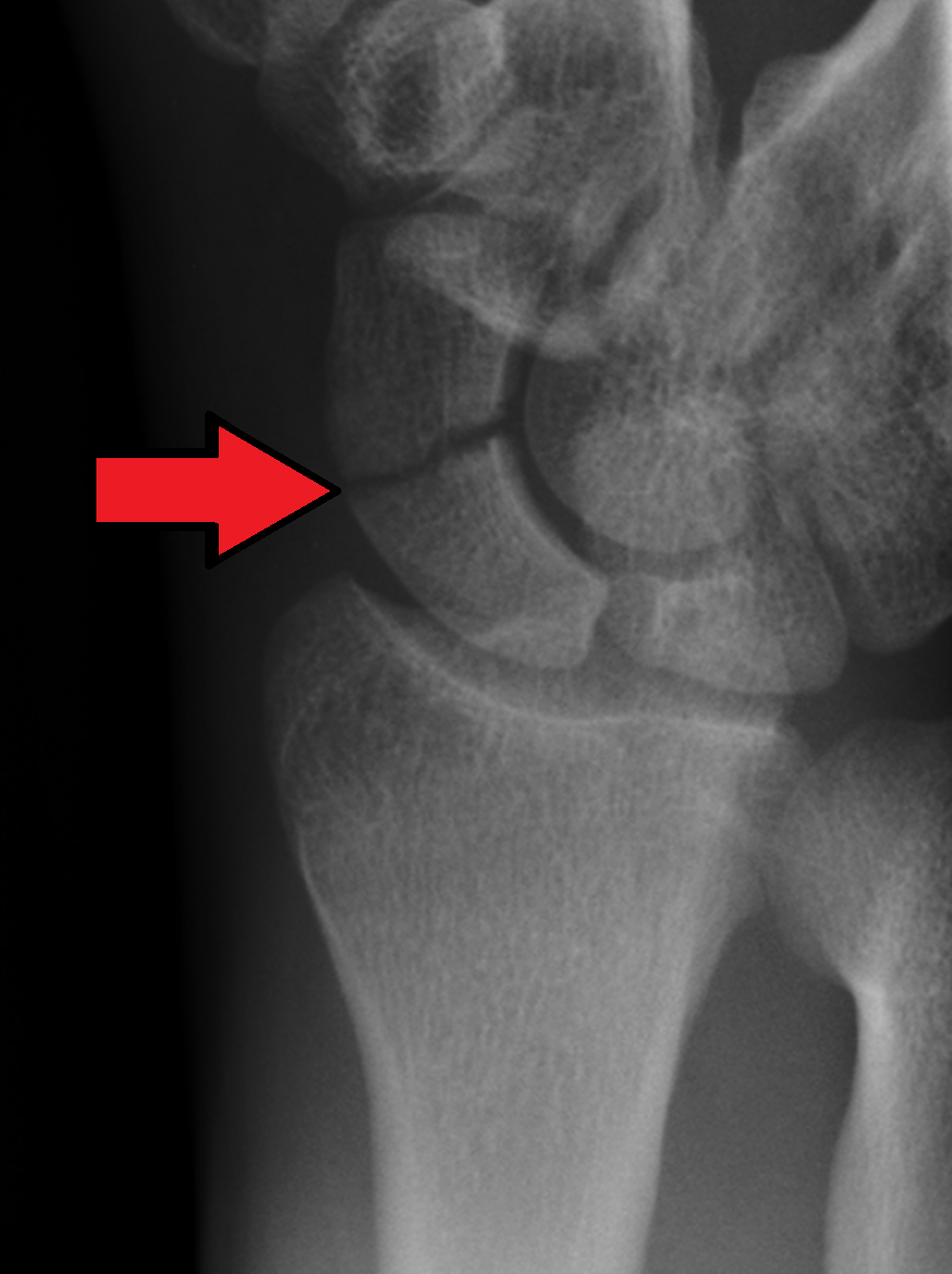
Scaphoid fracture Traumatic history of a fall on an outstretched hand with subsequent anatomical snuff box pain
High risk of nonunion leading to advanced collapse and significant disability
Typically confirmed by x-ray
Represents 60% of all carpal fractures (7)
Avascular necrosis Multifactoral causes, including skeletal variations, trauma, or diseases that affect vascular flow (i.e., lupus, sickle cell anemia, etc.)
Slowly progressive pain, stiffness, or swelling over the lunate
Avascular necrosis may affect any of the carpal bones but most commonly involves the lunate (aka Keinbock’s disease) (8)
Typically affects men between the ages 20-40

Inflammatory arthropathy Insidious onset, prolonged morning stiffness, and swelling
Often affecting multiple joints with potential skin and nail changes
Likely culprits include rheumatoid arthritis, psoriatic arthritis, pseudogout, and lupus
Diagnosed via lab testing (CBC, ESR, RA factor, HLA B27, ANA, etc.)
Pro Tip: Download the ChiroUp Inflammatory Arthropathy Quick Reference Card for a handy refresher. (Keep a copy handy in each treatment room.)

“Wrist trauma is one of the most common Emergency Department (ED) attendances and accounts for approximately 20 % of all injuries. 39 % of patients with wrist trauma have a fracture.” (9)
While not quite as sensitive as the Ottowa Ankle Rules, the counterpart Amsterdam Wrist Rules highlight several findings in acute wrist trauma patients that indicate a higher likelihood of fracture and may justify imaging. (9)
Distal radial tenderness (Odds Ratio- OR: 15.7)
Visible deformity (OR: 3.97)
Wrist swelling (OR: 7.92)
Snuffbox swelling (OR: 1.60)
Painful palmar flexion, supination, or radial deviation (OR: 1.90 - 2.25)
Painful radioulnar ballottement test/ i.e., shearing (OR: 1.76)
Male sex (OR: 1.46)
Increased age (OR: +1.04 per 10 years)
If initial radiographs are negative or equivocal, repeat radiographs in 10-14 days, MRI, or CT are usually appropriate as the follow-up imaging study. (10) For a deeper dive, the ACR Appropriateness Criteria® for Acute Hand and Wrist Trauma outlines the appropriateness of advanced imaging for clarifying complex fractures or defining occult fractures. (10)
The ACR Appropriateness Criteria® for Chronic Wrist Pain state that radiographs are indicated as the first imaging test in all patients with chronic wrist pain, regardless of the suspected diagnosis. (11)
Standard hand and wrist x-ray images include PA, PA oblique, and lateral views. (12) Additional considerations include:
A dedicated scaphoid view for patients with a history of trauma or snuffbox tenderness. (13-15)
An AP oblique view can highlight the pisiform by limiting triquetral overlap. (16)
Flexion, extension, and radial and ulnar deviation views can assess gross motion and decrease carpal superimposition. (12)
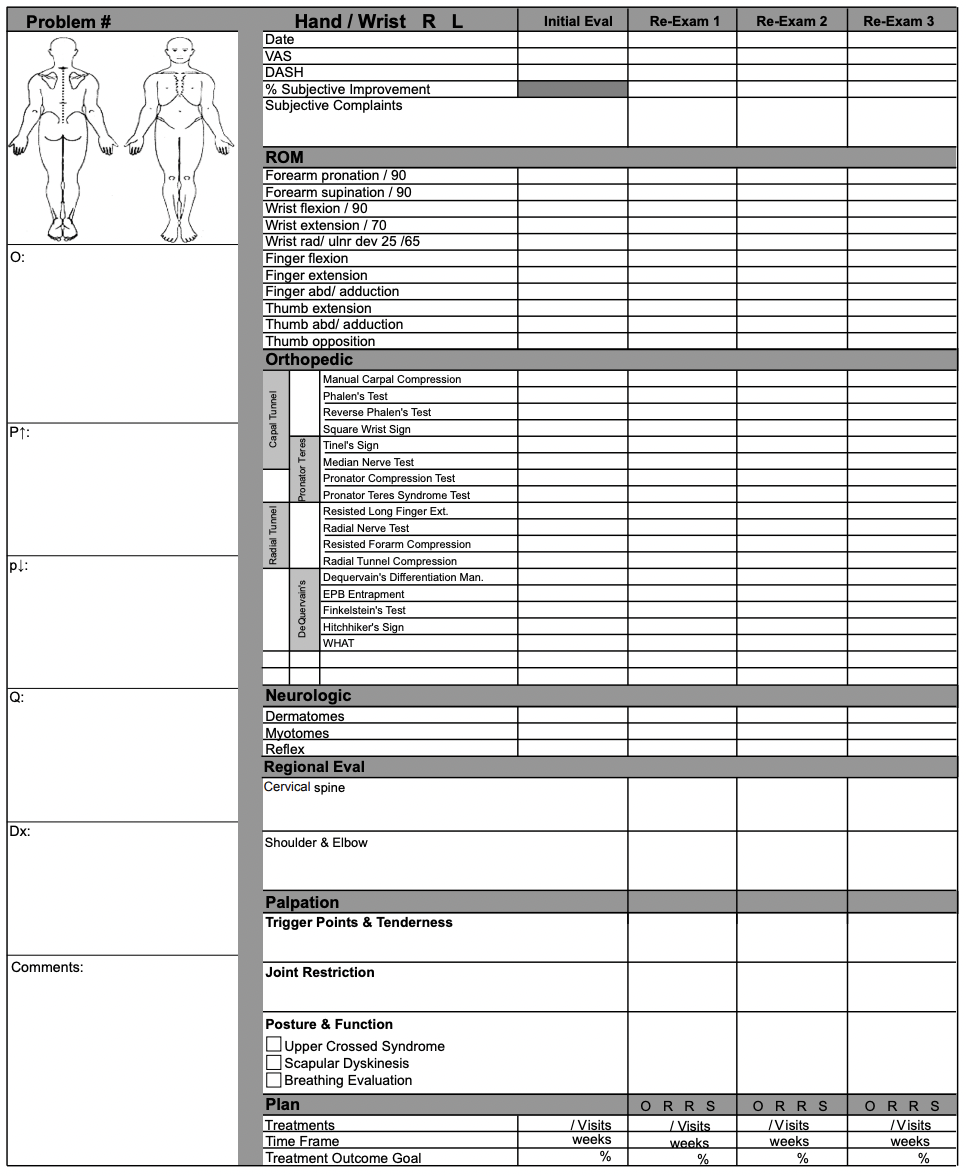
Download the ChiroUp Hand and Wrist evaluation form and every other regional exam form which can be found in your ChiroUp account in the Forms Library under clinical/regional exam forms.
Once you’ve nailed the diagnosis, you’ll have a better chance to apply the correct management for the right patient at the right time. ChiroUp subscribers can visit their Condition reference library for detailed best-practice synopses for more than 115 diagnoses, including many of the hand and wrist conditions listed above.
Need a functionality refresher? See how to use the ChiroUp condition reference library.
We’re honored to be your partner in automating clinical excellence! Together, we will become the undeniable best choice for patients and payors alike!
-
1. Avery DM, Rodner CM, Edgar CM. Sports-related wrist and hand injuries: a review. Journal of orthopaedic surgery and research. 2016 Dec;11(1):1-5. Link
2. Simpson AM, Donato DP, Veith J, Magno-Padron D, Agarwal JP. Hand and wrist injuries among collegiate athletes: the role of sex and competition on injury rates and severity. Orthopaedic journal of sports medicine. 2020 Dec 15;8(12):2325967120964622. Link
3. Almquist EE. Painful conditions of the forearm, wrist, and hand. In: Loeser JD, Bonica JD. Bonica’s Management of pain. 3d ed. Philadelphia: Lippincott Williams & Wilkins, 2001.
4. Ferrante MA. The relationship between sustained gripping and the development of carpal tunnel syndrome. Federal Practitioner. 2016 Jul;33(7):10. Link
5. Zambelis T, Tsivgoulis G, Karandreas N. Carpal tunnel syndrome: associations between risk factors and laterality. European neurology. 2010;63(1):43-7. Link
6. Rosedale R, Rastogi R, Kidd J, Lynch G, Supp G, Robbins SM. A study exploring the prevalence of Extremity Pain of Spinal Source (EXPOSS). Journal of Manual & Manipulative Therapy. 2020 Aug 7;28(4):222-30. Link
7. Steffes MJ. Scaphoid Fracture. Orthobullets. 7/14/21. Accessed online on 10/11/2022 at Link
8. Afshar A, Tabrizi A. Avascular necrosis of the carpal bones other than Kienböck disease. The Journal of Hand Surgery. 2020 Feb 1;45(2):148-52. Link
9. Walenkamp MM, Bentohami A, Slaar A, Beerekamp MS, Maas M, Jager LC, Sosef NL, van Velde R, Ultee JM, Steyerberg EW, Goslings JC. The Amsterdam wrist rules: the multicenter prospective derivation and external validation of a clinical decision rule for the use of radiography in acute wrist trauma. BMC musculoskeletal disorders. 2015 Dec;16(1):1-9. Link
10. Torabi M, Lenchik L, Beaman FD, Wessell DE, Bussell JK, Cassidy RC, Czuczman GJ, Demertzis JL, Khurana B, Klitzke A, Motamedi K. ACR Appropriateness Criteria® acute hand and wrist trauma. Journal of the American College of Radiology. 2019 May 1;16(5):S7-17. Link
11. Rubin DA, Roberts CC, Bencardino JT, Bell AM, Cassidy RC, Chang EY, Gyftopoulos S, Metter DF, Morrison WB, Subhas N, Tambar S. ACR appropriateness criteria® chronic wrist pain. Journal of the American College of Radiology. 2018 May 1;15(5):S39-55. Link
12. Copeland J, Byerly DW. Wrist Imaging. InStatPearls [Internet] 2021 Apr 28. StatPearls Publishing. Link
13. Phillips TG, Reibach AM, Slomiany WP. Diagnosis and management of scaphoid fractures. Am Fam Physician. 2004 Sep 01;70(5):879-84. Link
14. Jain R, Jain N, Sheikh T, Yadav C. Early scaphoid fractures are better diagnosed with ultrasonography than X-rays: A prospective study over 114 patients. Chin J Traumatol. 2018 Aug;21(4):206-210. Link
15. Meyer P, Lintingre PF, Pesquer L, Poussange N, Silvestre A, Dallaudiere B. Imaging of Wrist Injuries: A Standardized US Examination in Daily Practice. J Belg Soc Radiol. 2018 Jan 31;102(1):9. Link
16. Bhat AK, Kumar B, Acharya A. Radiographic imaging of the wrist. Indian J Plast Surg. 2011 May;44(2):186-96. Link