Insular lobe anatomy
•Download as PPTX, PDF•
2 likes•753 views
This document provides an overview of the anatomy of the insula and sylvian fissure. It describes the insula as the 5th lobe of the brain, located deep within the sylvian fissure hidden by the frontal, parietal, and temporal opercula. The document outlines the surgical anatomy of the insula including its pyramidal shape, surfaces, gyri, and relations to surrounding structures like the external capsule and internal capsule. It also discusses the arterial supply to the insula from the middle cerebral artery and various surgical approaches to access the insula like trans-sylvian and transcortical techniques.


























Insular lobe anatomy
- 1. Anatomy Of Insula and Sylvian Fissure PRESENTED BY DR ANKIT JAIN
- 2. HISTORY • The island or insula of Reil is named after the German anatomist, physiologist and psychiatrist, Johann Christian Reil (1759– 1813), who in 1809 first described this anatomically and functionally complex structure situated in the depth of the Sylvian fissure and hidden by the opercula of the frontal, parietal and temporal lobes
- 3. SURGICAL ANATOMY • 5th lobe of brain. • Mesocortical structure , link between allocortex and neocortex. • Part of para limbic system
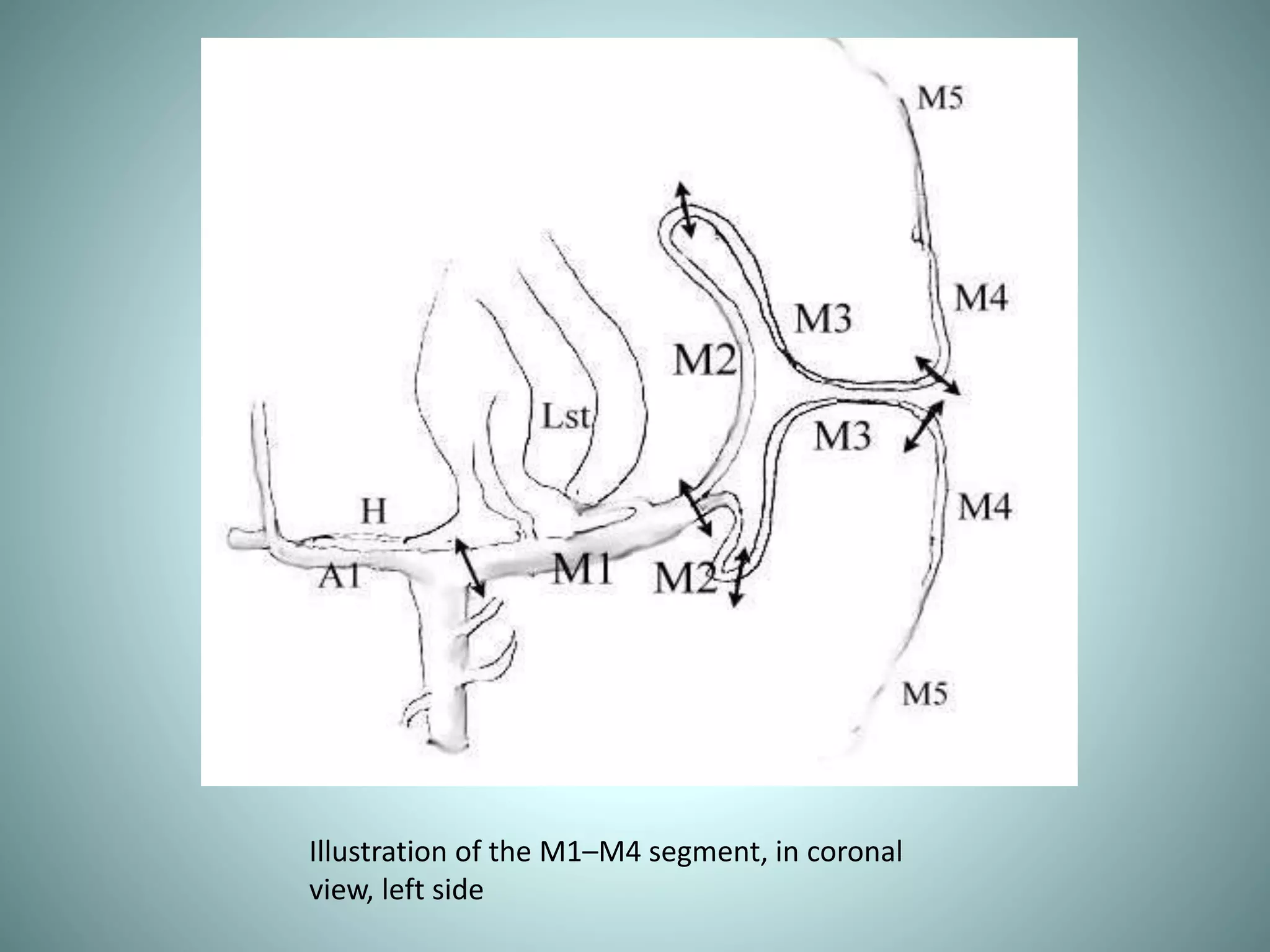
- 6. Illustration of the M1–M4 segment, in coronal view, left side
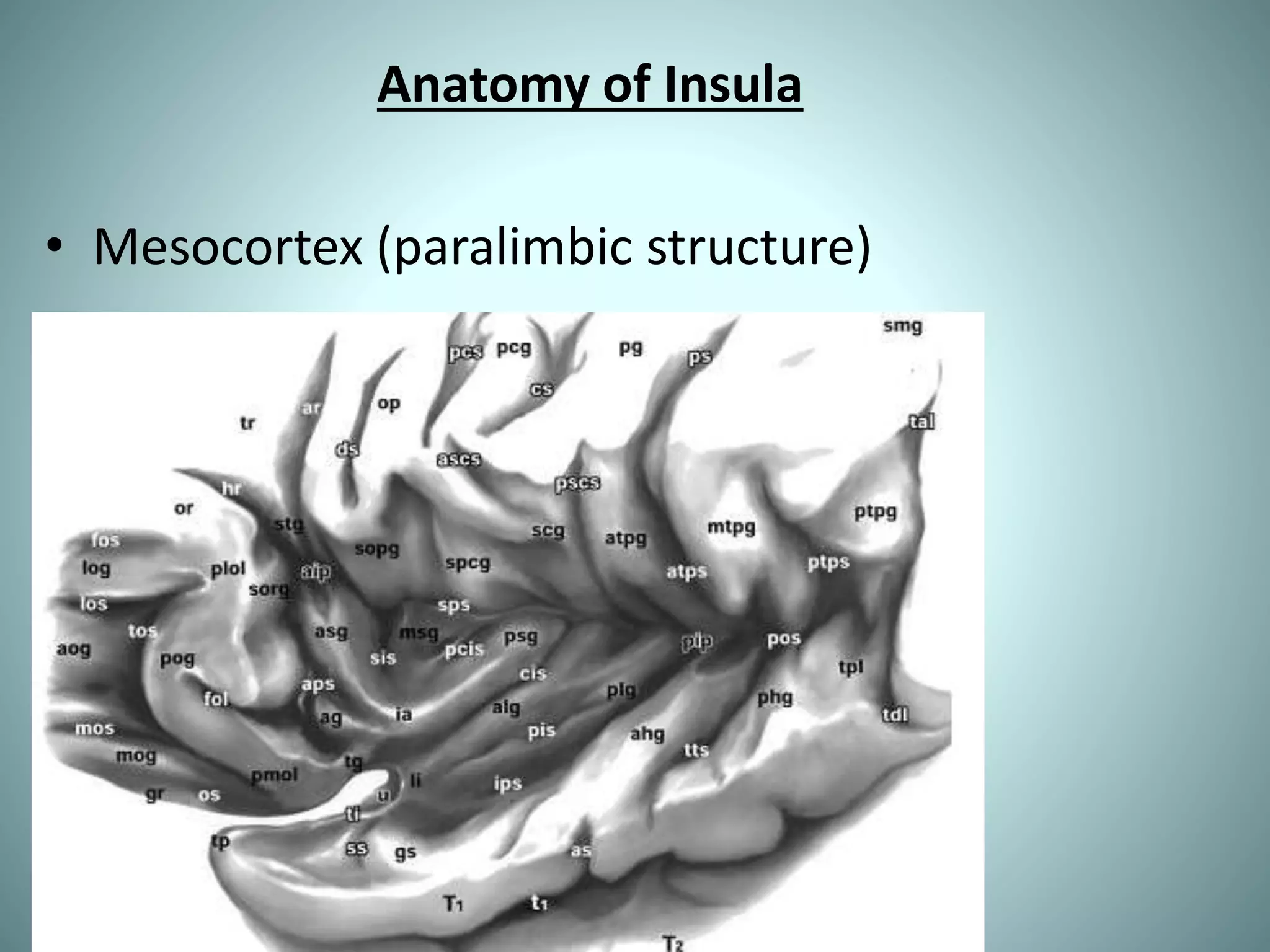
- 7. Anatomy of Insula • Mesocortex (paralimbic structure)
- 8. SURGICAL ANATOMY • A well-defined cerebral cortical surface • Pyramidal in shape. • Base medially. • 3 surfaces. • Hidden by frontal temporal and parietal operculum.
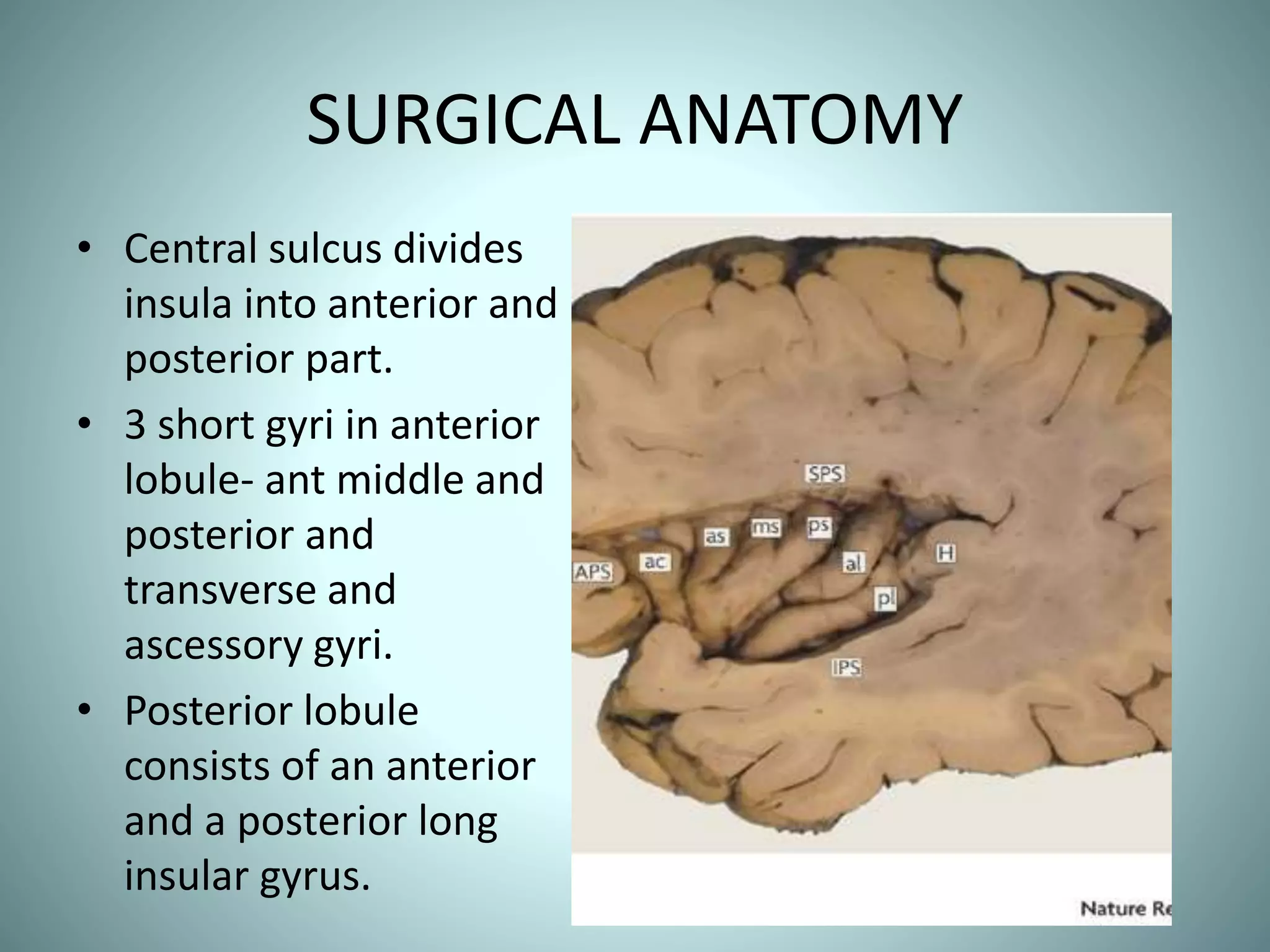
- 9. SURGICAL ANATOMY • Central sulcus divides insula into anterior and posterior part. • 3 short gyri in anterior lobule- ant middle and posterior and transverse and ascessory gyri. • Posterior lobule consists of an anterior and a posterior long insular gyrus.
- 10. SURGICAL ANATOMY
- 13. SURGICAL ANATOMY • EXTREME CAPSULE • CLAUSTRUM • EXTERNAL CAPSULE • LENTIFORM NUCEUS • INTERNAL CAPSULE
- 15. SURGICAL ANATOMY • M1- LATERAL LENTICULOSTRIATE ARTRIES. • M2 – SHORT PERFORATORS. LONG PERFORATORS.
- 16. SURGICAL ANATOMY. • Lateral Lenticulostriate Arise from M1. 1- 15 in number. 0.5-1.5 mm in diameter. Supply Internal capsule and Lentiform nucleus. Related to Limen insulae(1.5 cms). May supply insula.
- 17. SURGICAL ANATOMY • M2 PERFORATORS Short and medium perforators supply insula and can be sacrificed. Long perforators – arise in the postero superior part of insula and supply corona radiata.
- 18. Limen Insulae • The limen insulae is a slightly raised, arched ridge located at the junction of the sphenoidal and operculoinsular compartments of the sylvian fissure and extends from the temporal pole to the orbital surface of the frontal lobe • LIMEN RECESS: between the medial border of the limen insulae and the lateral limit of the anterior perforated substance, which isthe point of entrance of the most lateral LSA : MEDIAL BORDER OF RESECTION
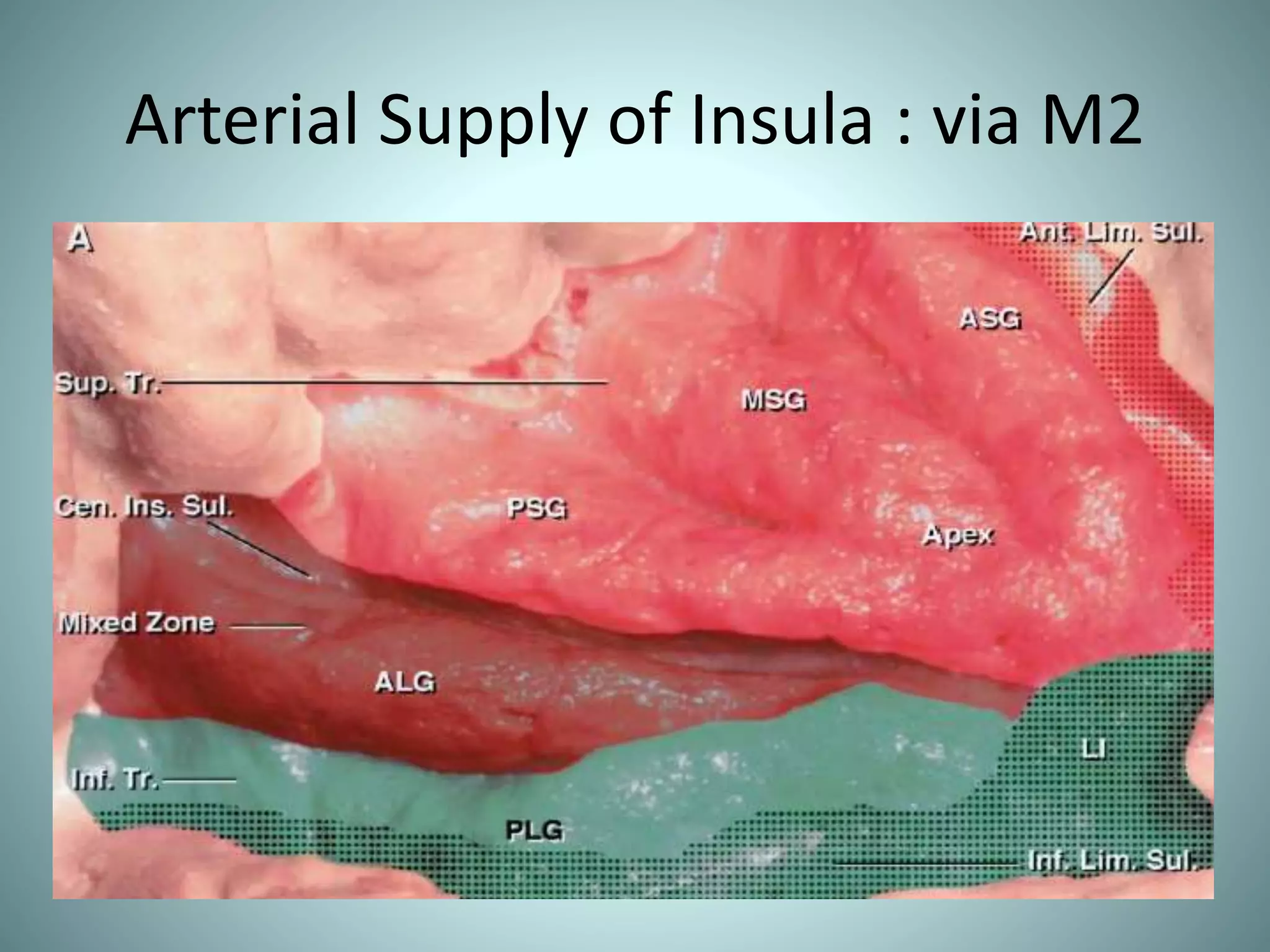
- 20. Arterial Supply of Insula : via M2
- 21. The limen area, inferior limiting sulcus, long gyri, and central insular sulcus are drained by the deep MCV (purple area). The SSV drained the middle short gyrus and insular apex more commonly than any other insular area (light blue area). The transitional zone, which is usually drained by both the superficial and deep venous systems, included the anterior and posterior short gyri and the anterior limiting sulcus (stippled area).
- 22. Functions • Insular language area • Cognitive control of emotions • Consciousness • Pain perception Relations - To the sylvian fissure - To the Cerebral fibre system and basal ganglia - To the Lateral ventricle
- 23. Relation to the fibres
- 24. Relation to the lateral ventricle The foramen of Monro is located deep to the middle portion of the posterior short gyrus. The posterior end of the insula and the junction of superior and inferior limiting sulci are located superficial to the anterior edge of the atrium.
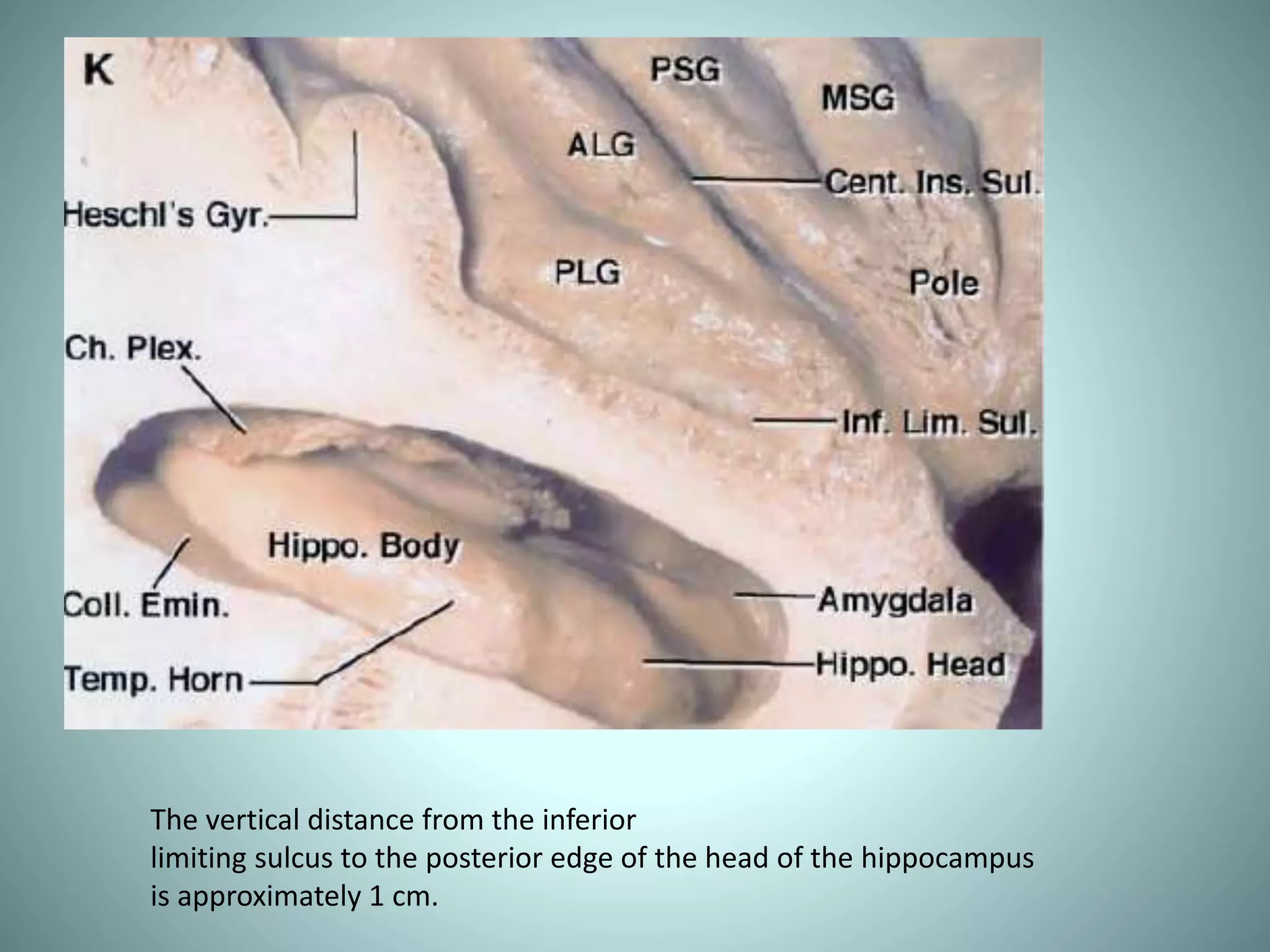
- 25. The vertical distance from the inferior limiting sulcus to the posterior edge of the head of the hippocampus is approximately 1 cm.
- 26. CLASSIFICATION TYPE LOCATION SUBCATEGORY 1 TEMPORAL MEDIOBASAL a.Medial temporal pole. b.Amygdalar. c.Hippocampal. d.Parahippocampal. 2 Cingulate Gyrus a. anterior. b. Middle. c. Posterior. 3 Insular and parainsular a. Pure Insular anterior posterior entire b. Insular frontobasal c. Insular temporomediobasal. d. Insular forntobasal- temporomediobasal 4 Medial limbic association areas a. Fornicial b. Septal c. mamillary 5 Entire limbic system
- 27. BERGER AND SANAI CLASSIFICATION ZONE 1 – Antero superior ZONE 2- Postero superior. ZONE 3 – Postero inferior. ZONE 4- Antero inferior GIANT- Involving all zones
- 30. SURGICAL APPROACHES • TRANS-SYLVIAN. • TRANSCORTICAL
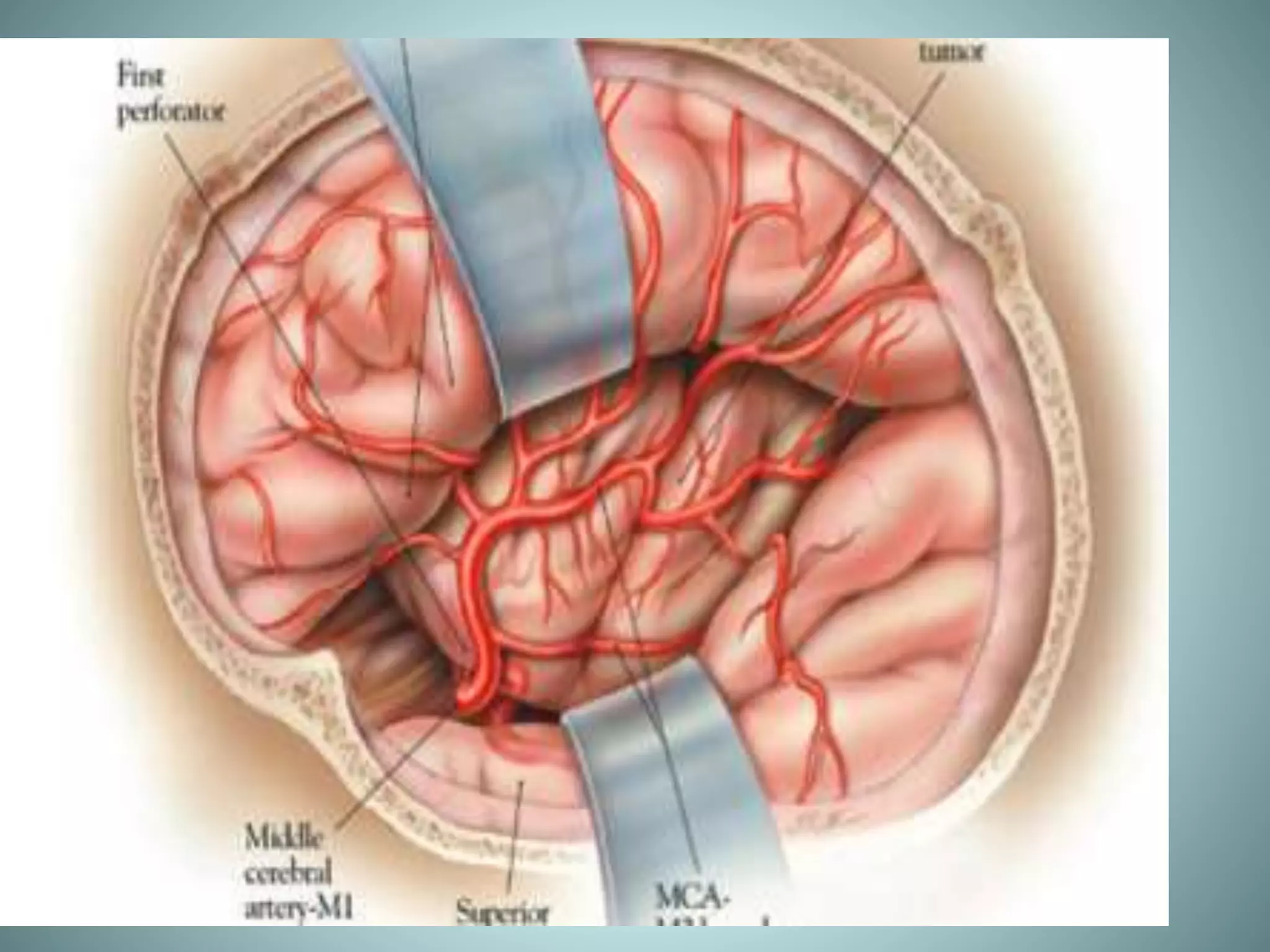
- 31. TRANSYLVIAN APPROACH. Pioneered by Yasargil Most suitable for purely insular gliomas Wide exposure. Tumor devascularisation. Less chance of injury to eloquent structures DISADVANTAGES: Wide retraction required retraction related temporary deficits. Chances of vascular injury more. Vasospasm.
- 34. TRANSCORTICAL APPROACH • Most appropriate for tumors with opercular spread. • Avoids injuries to vessels while maintaining dissection with in pia. • Less chance of vasospasm. • Need for preoperative functional MRI and intraop cortical mapping. • Trans cortical windows are created through the nonfunctional cortex above and below the sylvian fissure-Window technique.
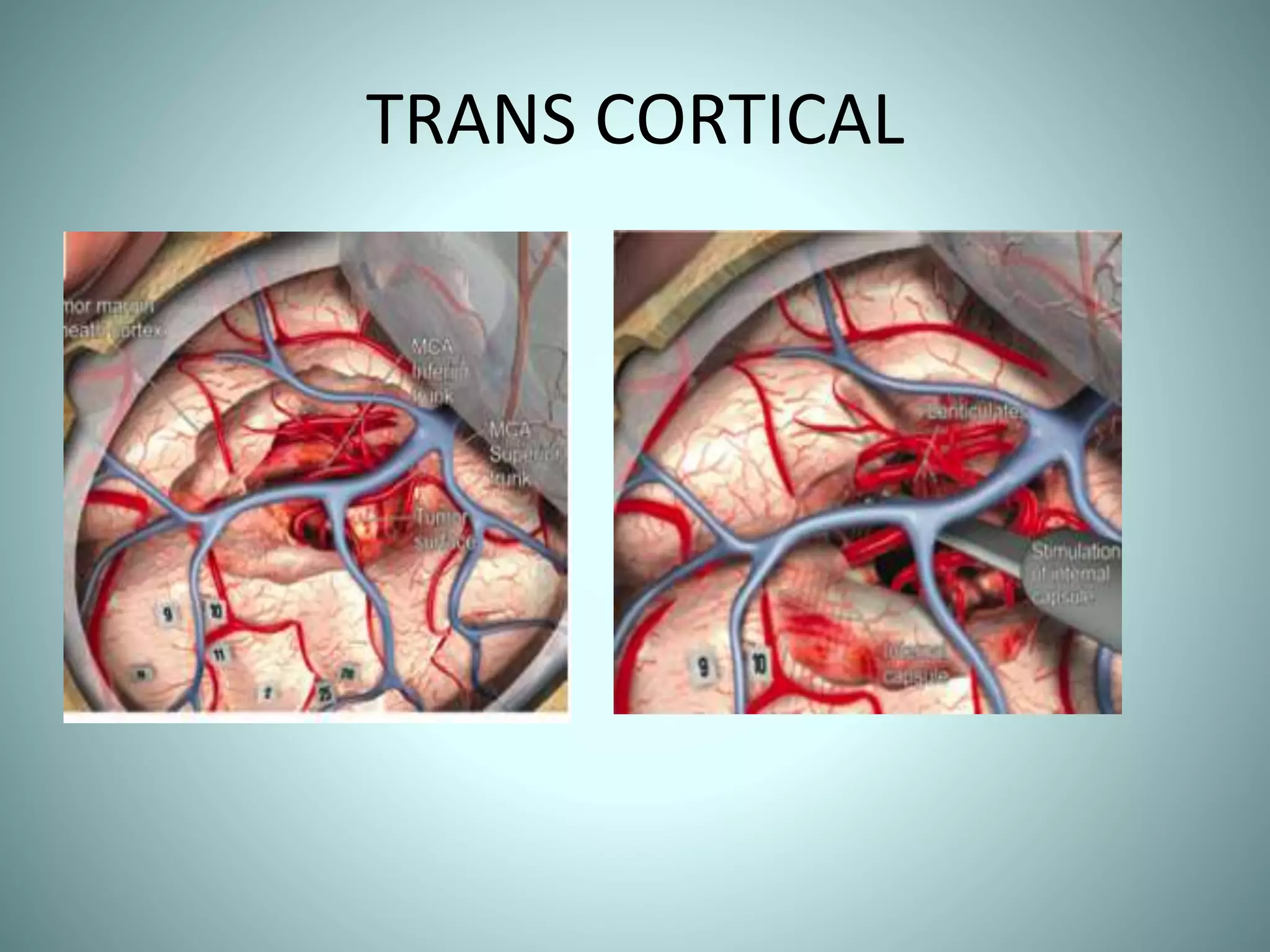
- 35. TRANS CORTICAL
- 36. COMPLICATIONS • HEMIPARESIS. • APHASIA • VISUAL DEFICITS. • NEURO PSYCHOLOGICAL WORSENING.
- 37. THANK YOU