Myofascial pain dysfunction (mpd)
•Download as PPTX, PDF•
5 likes•781 views
Myofascial pain dysfunction (MPD) is a temporomandibular disorder characterized by pain in the muscles of mastication. Typical features include intermittent dull facial pain that worsens throughout the day, with pain increasing during chewing or stress. MPD is diagnosed based on a history of unilateral facial pain and physical exam findings like tenderness in the masticatory muscles and limited jaw movement. Conservative treatments include reassurance, splint therapy, physical therapy, and medications like NSAIDs or muscle relaxants. More invasive options may include injections or orthodontic/jaw surgery if conservative measures fail.


































Myofascial pain dysfunction (mpd)
- 1. Myofascial Pain dysfunction (MPD) Dr jameel kifayatullah
- 2. Myofascial Pain dysfunction (MPD) • Temporomandibular disorder is defined as "musculoskeletal disorders affecting the temporomandibular joints and their associated musculature. It is a collective term which represents a diverse group of pathologies involving the temporomandibular joint, the muscles of mastication, or both"
- 3. SYNONYMS Temporomandibular joint pain dysfunction syndrome Temporomandibular pain dysfunction syndrome Temporomandibular joint syndrome Temporomandibular dysfunction syndrome Temporomandibular dysfunction, Temporomandibular disorder, Temporomandibular syndrome, Facial arthromyalgia, Myofacial pain dysfunction syndrome, Craniomandibular dysfunction (CMD), Myofacial pain dysfunction, Masticatory myalgia, Mandibular dysfunction Costen's syndrome.
- 4. Typical features • intermittent dull aching facial pain • worsen throughout the day(characteristic of MPD) • Pain increases with mastication or Stress • Onset gradual • Most patients in between 16 and 40 years • Female preponderence 4:1 • Pain typically felt infront of ear • Pain usually one sided
- 5. Typical features • Limitation of mouth opening • Clicking or crepitus in the joint
- 6. Laskin Diagnostic criteria Cardinal symptoms • The most common finding is pain of unilateral origin • The next most common finding is mastictory muscle tenderness • The third most common symptom is a clicking or popping noise in the TMJ • Limitation of jaw function is the fourth cardinal symptom of the pain-dysfunction syndrome
- 8. LASKIN DIAGNOSTIC CRITERIA • Negative characteristics: 1)Absence of clinical, radiographic, or biochemical evidence of organic changes in the TMJ 2)Lack of tenderness in the TMJ when this area is palpated via the external auditory meatus. Etiology of the pain-dysfunction syndrome .Daniel M Laskin .JADA.
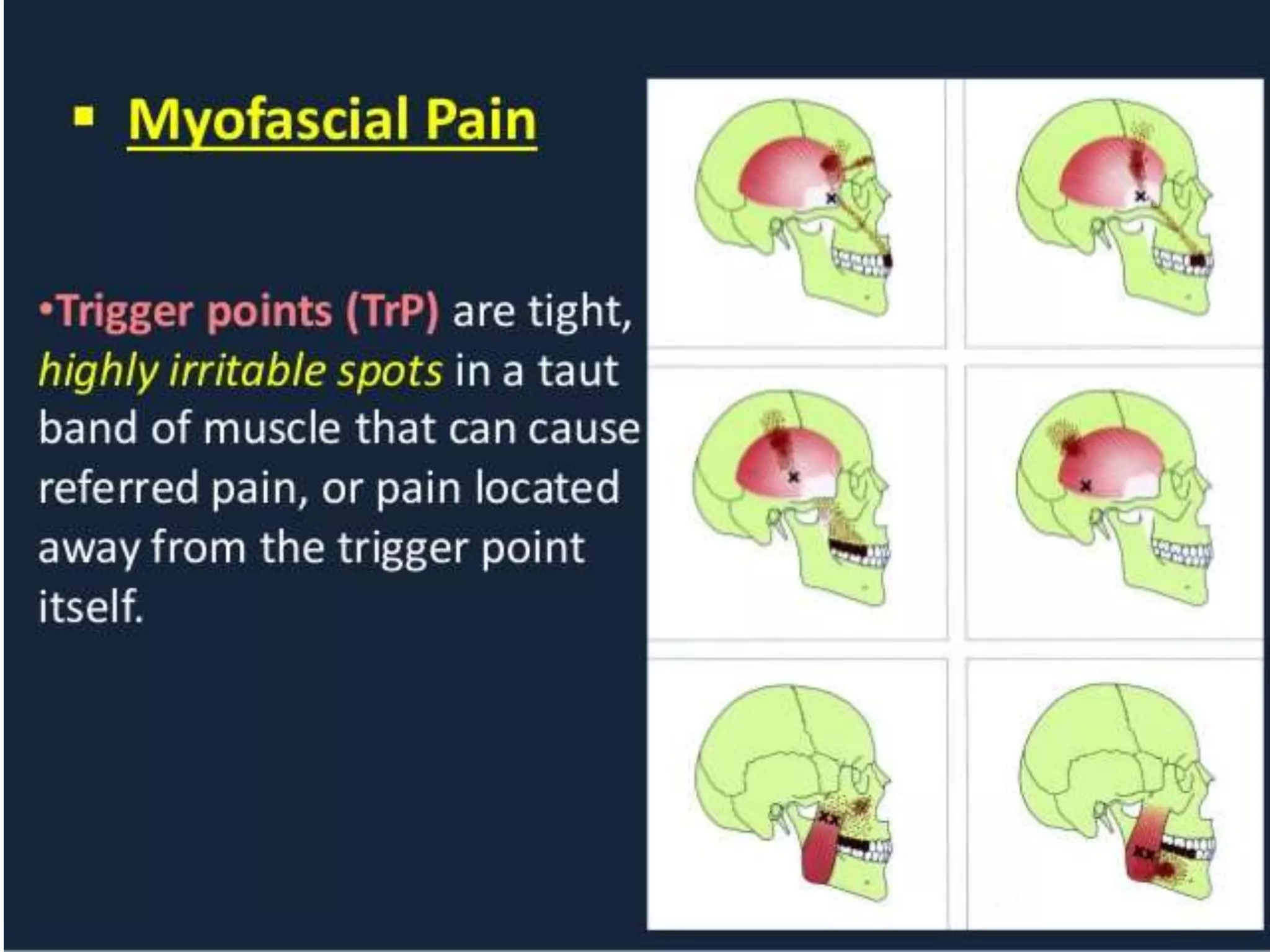
- 9. Myofascial trigger points • Hyperirritable locus within a taut band of skeletal muscle that is located in muscular tissue or in its associated fascia or tendon • MPD can also be accompanied by myofascial trigger points • This spot is painful on compression and can evoke characteristic referred pain and autonomic phenomena
- 12. Etiology of MPDS Multifactorial • Stress • anxiety • Bruxism • Clenching • Malocclusion • Parafunctional oral habbits • Internal derangement of TMJ • Rheumatologic diseases(polymyalgia rheumatica) • Fibromyalgia • Vasculitis(temporal arteritis)
- 15. Clinical evaluation • History: unilateral facial pain Radiation : pain may radiate to ear,temporal and periorbital regions,angle of mandible and back of the neck Nature of pain: Dull ,constant ache that is worse at certain times during the day Limited jaw motion Attempt at active motion (yawning, chewing,talking) Increase the pain
- 16. Clinical Evaluation • History locking of jaw either in closed mouth position with an inability to open it locking of jaw in open mouth position with an inability to close the jaw symptoms worse in the morning particularly in patients who grind their teeth during sleep Parafunctional habbits common
- 17. examination • Inspection: deviation of mandible to the affected side on opening clicking or popping noise in the joint Physical examination Maximal interincisal opening,lateral movements ,protrusion measurements Palpation of muscles of mastication
- 18. Physical examiantion • Examination of cervical muscles • Palpation and auscultation of TMJ • Examination of oral cavity,dentition,occlusion, • Examination of salivary glands • Inspection and palpation of anterior and posterior aspects of the neck • Auscultation of carotids • Examination of cranial nerves
- 19. Findings in physical examination • Noise in TMJ on mandibular movement • Muscle tenderness producing pain or discomfort on palpation of masticatory muscles • Tenderness in anterior meck muscles(suprahyoid and sternocleidomastoid) • Tenderness in posterior cervical paraspinal muscles(semispinalis capitis, splenius capitis,and suboccipital muscles)
- 20. Findings on physical examination • Tenderness in upper shoulder muscles( trapezius anf levator scapulae) • Mandibular hypomobility and deviation on opening
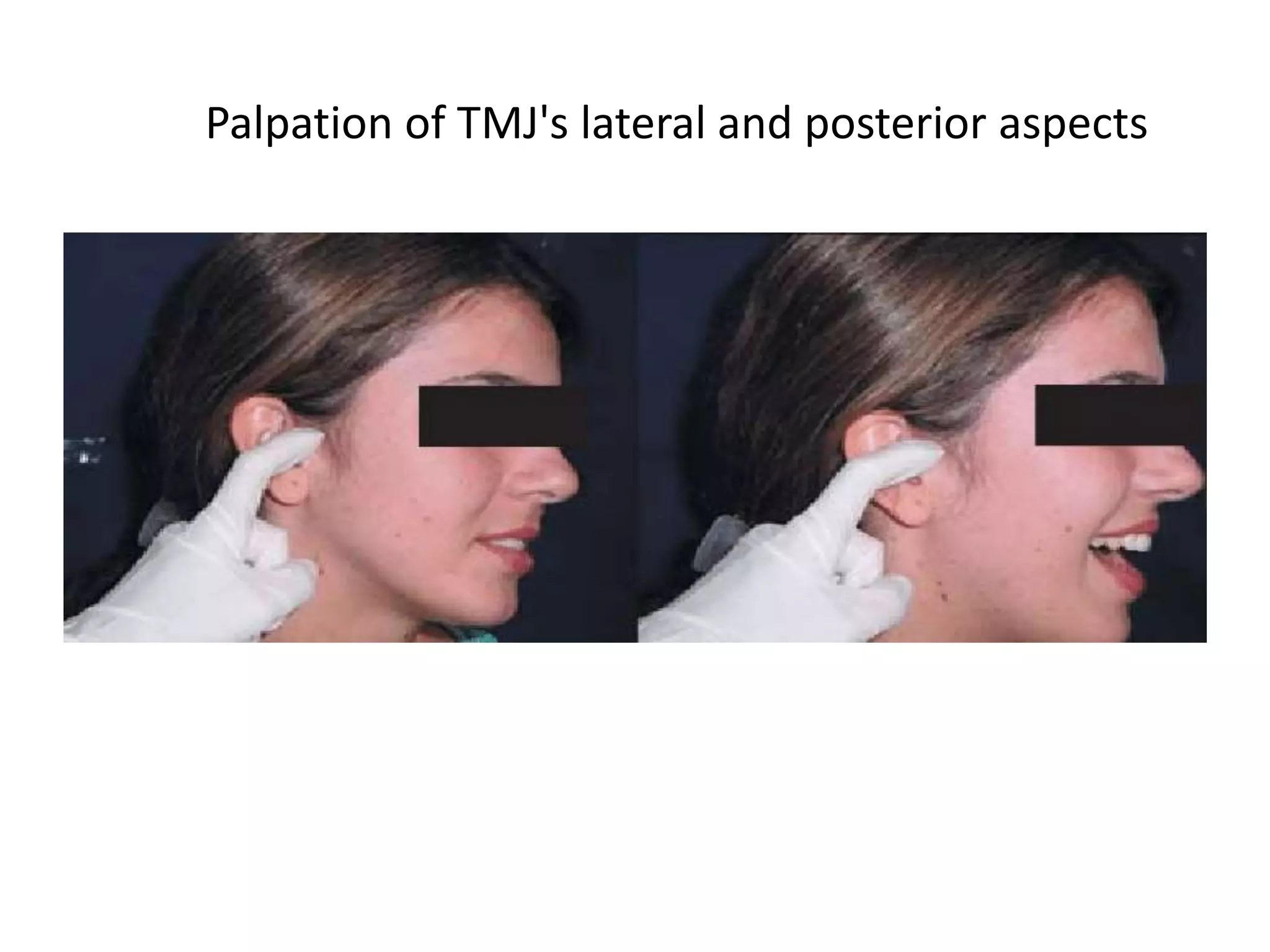
- 21. Palpation of TMJ's lateral and posterior aspects
- 22. Palpation of the superficial and deep masseter muscle
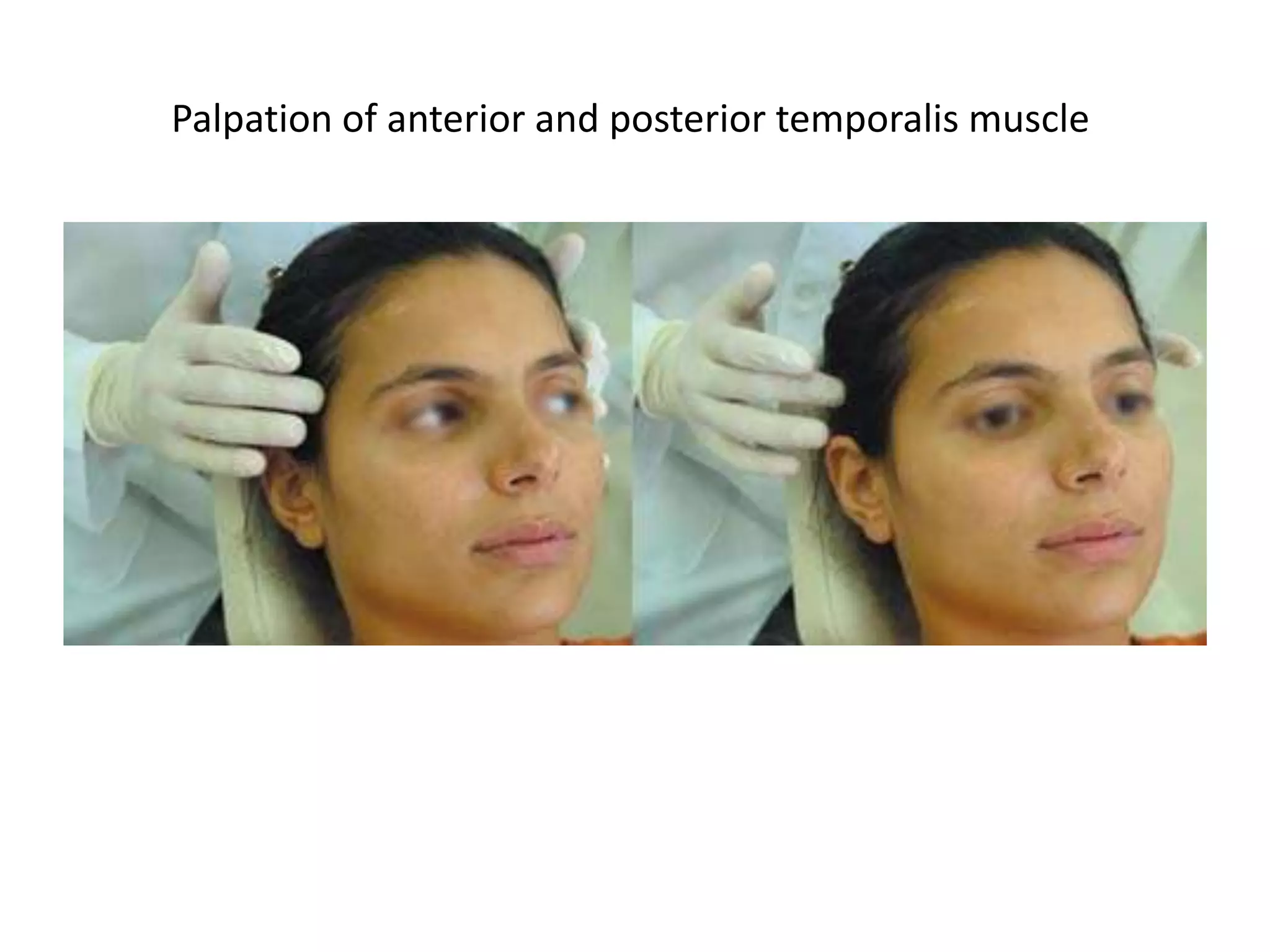
- 23. Palpation of anterior and posterior temporalis muscle
- 25. Measurement of maximum active opening and maximum lateral movement
- 26. Joint sound inspection with a stethoscope
- 27. Blood chemistry • Blood and serum inflammatory markers to rule out autoimmune and vasculitis)
- 28. CLINICAL EVALUATION • IMAGING • DIAGNOSTIC NERVE BLOCKS • TRIGGER POINT INJECTIONS • DENTAL MODELS FOR MAXILLOMANDIBULAR ANALYSIS
- 30. NERVE BLOCK
- 31. management Principles of management of pain dysfunction syndrome • Exclude joint disease • Exclude giant cell arteritis • Exclude pain and infection of dental origin • Reassurance and education • Conservative management-reversible treatments only • Soft diet and jaw exercises • Consider need for a splint • Analgesics or anxiolytics in selected cases
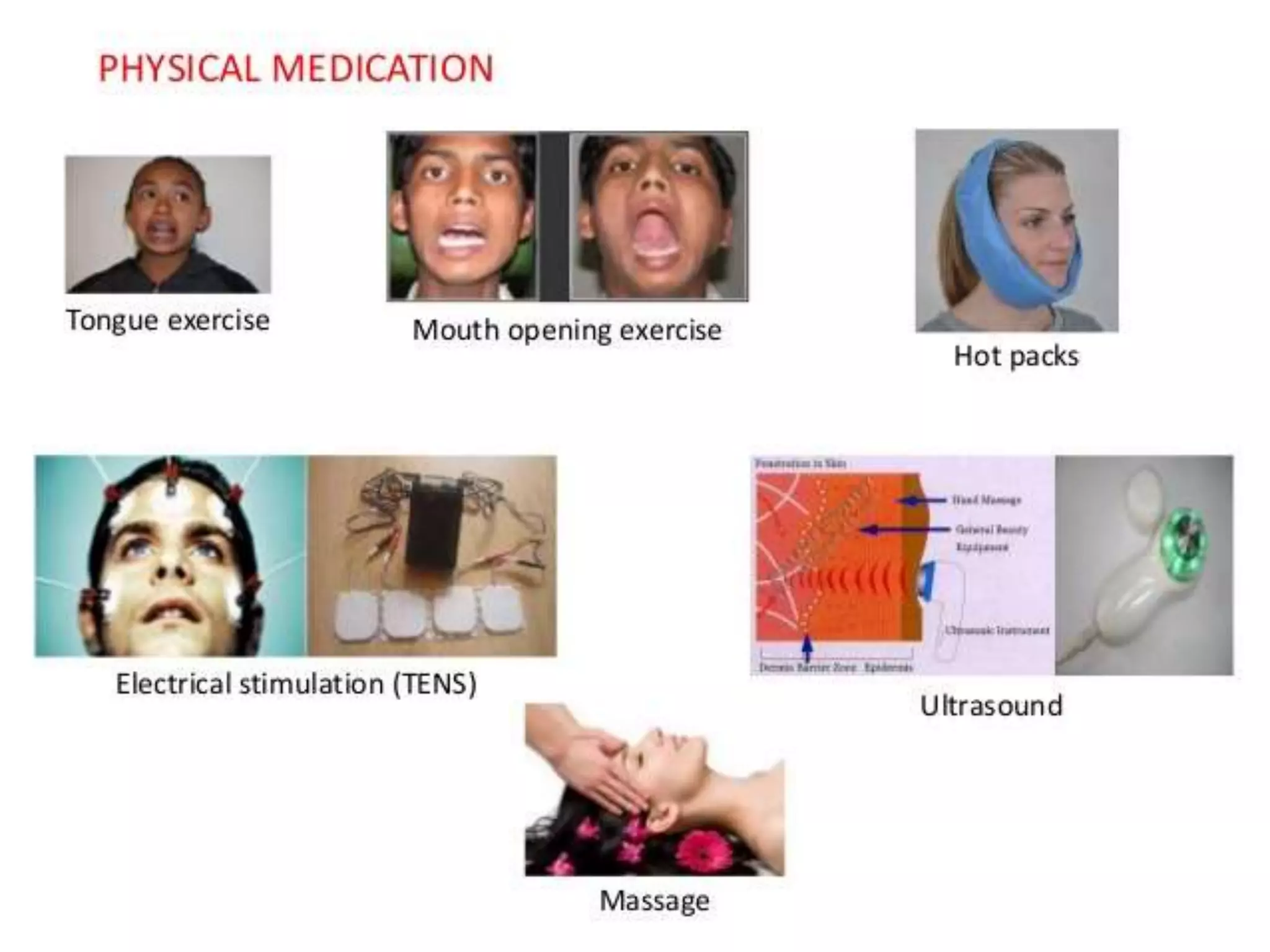
- 33. Treatment options generic approach using several modalities • Reassurance • Stress management (relaxation exercises,biofeedback) • Occlusal splint therapy • Physical therapy(TENS,Massage,exer cise program) • Application of heat to affected muscles • NSAIDS • MUSCLE RELAXANTS • ANXIOLYTICS • Anticonvulsants • Botox • Trigger point injections • Vapocoolant spray
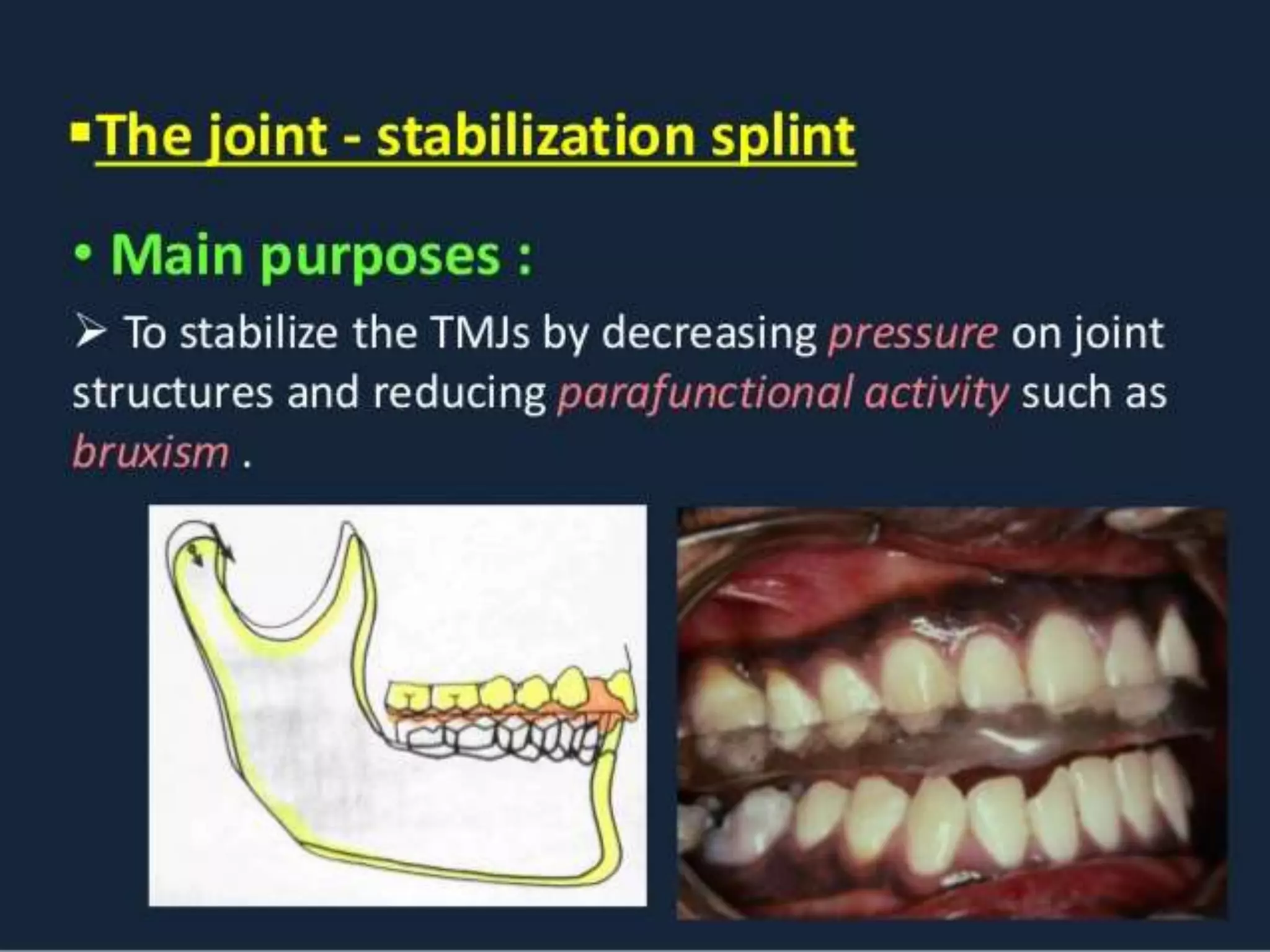
- 39. OCCLUSAL SPLINT • OCCLUSAL SPLINT: simple flat plane splint that covers all the teeth, and all the teeth should touch the splint evenly in centric occlusion and in centric relationship • Splint should have a shallow anterior guidance that separates the teeth during excursive movements • The concept is to give rest to the muscles and to decrease TMJ loading
- 40. INVASIVE TREATMENT MODALITY • PATIENTS NOT RESPONDING TO CONSERVATIVE THERAPY WITH AN OCCLUSAL SPLINT HAVING SIGNIFICANT MALOCCLUSIONORTHODONTIC TREATMENT OR ORTHOGNATHIC SURGERY(TX MODALITY)
- 41. OTHER MODALITIES • Trigger point injections:local anaesthetic with or without steroid injected directly into tender areas in the muscles • Botulinum Toxin: MPD improved with injection of botulinum into muscle to reduce muscle activity