Emesis and anti emetic drugs
•Download as PPTX, PDF•
57 likes•8,720 views
This document discusses the pathophysiology of vomiting and its control. It begins by outlining the various central and peripheral mechanisms that can trigger vomiting, including inputs from the vestibular system, enteric nervous system, and various visceral afferents. It then describes the receptors and neurotransmitters involved, including 5-HT3, dopamine D2, muscarinic, and histamine H1 receptors. Common antiemetic drugs are grouped based on their mechanisms of action, such as 5-HT3 antagonists and antihistamines. The roles of various drug classes like phenothiazines, neurokinin-1 antagonists, and cannabinoids are explained. Antiemetic treatment for nausea and vomiting





































Emesis and anti emetic drugs
- 6. Inputs from the vestibular system of the inner ear. • Motion sickness. • Via vestibulocochlear nerve • Involvement of H1 type of histamine receptors in this system The enteric nervous system also transmits signals to the brain via the vagus nerve. • Activation of 5-HT3 receptors leading to vomiting • Drug induced vomiting • Gag reflex: pharyngeal stimulation of vagus nerve
- 7. Visceral afferents from the gastrointestinal tract (vagus or sympathetic nerves) - these signals inform the brain of such conditions as gastrointestinal distention (a very potent stimulus for vomition) and mucosal irritation. Visceral afferents from outside the gastrointestinal tract - this includes signals from bile ducts, peritoneum, heart and a variety of other organs. Afferents from extramedullary centers in the brain - it is clear that certain psychic stimuli (odors, fear), vestibular disturbances (motion sickness) and cerebral trauma can result in vomition. The chemoreceptor trigger zone
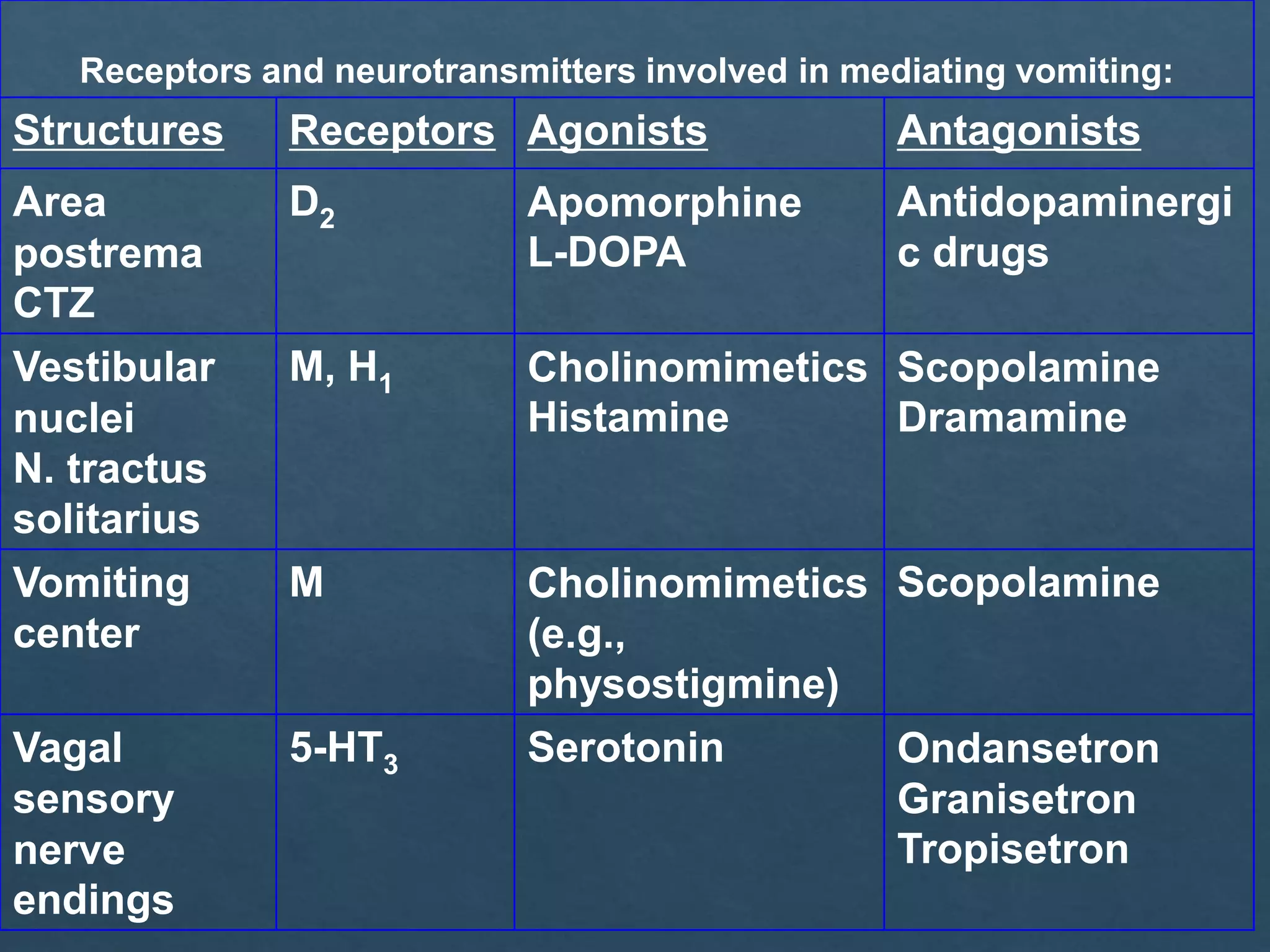
- 8. Receptors and neurotransmitters involved in mediating vomiting: Structures Receptors Agonists Antagonists Area postrema CTZ D2 Apomorphine L-DOPA Antidopaminergi c drugs Vestibular nuclei N. tractus solitarius M, H1 Cholinomimetics Histamine Scopolamine Dramamine Vomiting center M Cholinomimetics (e.g., physostigmine) Scopolamine Vagal sensory nerve endings 5-HT3 Serotonin Ondansetron Granisetron Tropisetron
- 9. Vomiting Centre (medulla) Cerebral cortex Anticipatory emesis Smell Sight Thought Vestibular nucleiMotion sickness Pharynx & GIT Chemo & radio therapy Gastroenteritis Chemoreceptor Trigger Zone (CTZ) (Outside BBB) Cancer chemotherapy Opioids Muscarinic, 5 HT3 & Histaminic H1 5 HT3 receptors Dopamine D2 5 HT3,, Opioid Receptors Muscarinic Histaminic H1 Pathophysiology of Emesis
- 10. NAUSEA RETCHING VOMETING An unpleasant sensation that immediately precedes vomiting Labored spasmodic respiratory movements against a closed glottis with contractions of the abdominal muscles, chest wall and diaphragm Intense contraction of the abdominal muscles and relaxation of the upper esophageal sphincter Rapid and forceful evacuation of stomach contents up to and out of the mouth
- 19. Groups Drugs Selective 5-HT3 Antagonists Ondansetron, Granisetron, Palonosetron & Dolasetron. D2 Antagonists • Substituted Benzamides Metoclopramide • Butyrophenones Domperidone • Neuroleptics Chlorpromazine, Triflupromazine, Prochlorperazine, H1 Antihistaminics Promethazine, Diphenhydramine, Dimenhydrinate, Doxylamine Anticholinergics Hyoscine, Dicyclomine
- 20. Cannabinoids Dronabinol , Nabilone Glucocorticoids Dexamethasone, Methylprednisolone Benzodiazepines Diazepam , Lorazepam Neurokinin-I Antagonist Aprepitant (oral formulation), Fosaprepitant (IV formulation)
- 28. D2 antagonism: Central antidopaminergic (D2) action of metoclopramide on CTZ 5-HT4 agonism: It acts in the GIT to enhance Ach release from the myenteric motor neurons 5HT3 antagonism: At higher concentrations it blocks 5HT3 receptors in the inhibitory myentric interneurons and in the CTZ
- 35. Neuroleptics Phenothiazines: Prochlorperazine Promethazine Triflupromazine Phenothiazines are antipsychotics with potent antiemetic property due to D2 antagonism and anti-muscarinic properties H1 and antihistaminic property. Most of these drugs produce significant degree of sedation. Acute muscle dystonia may occur
- 43. Domperidone (X) The combination of pyridoxine 10 mg and doxylamine 10 mg was withdrawn from the market due to increased risk of birth defects with the combination. Doxylamine/pyridoxine: • The only FDA-approved drug for treating nausea and vomiting in pregnancy • A greater form of reduction in Hyperemesis gravidarum • No teratogenic potential Ondansetron : • Class B safety in pregnancy • Most common parenteral and oral antiemetic used due to its efficacy Anticholinergics may be used as supportive drugs. Ginger capsules: 250 mg taken 4 times a day have been demonstrated to be effective against nausea and vomiting of pregnancy
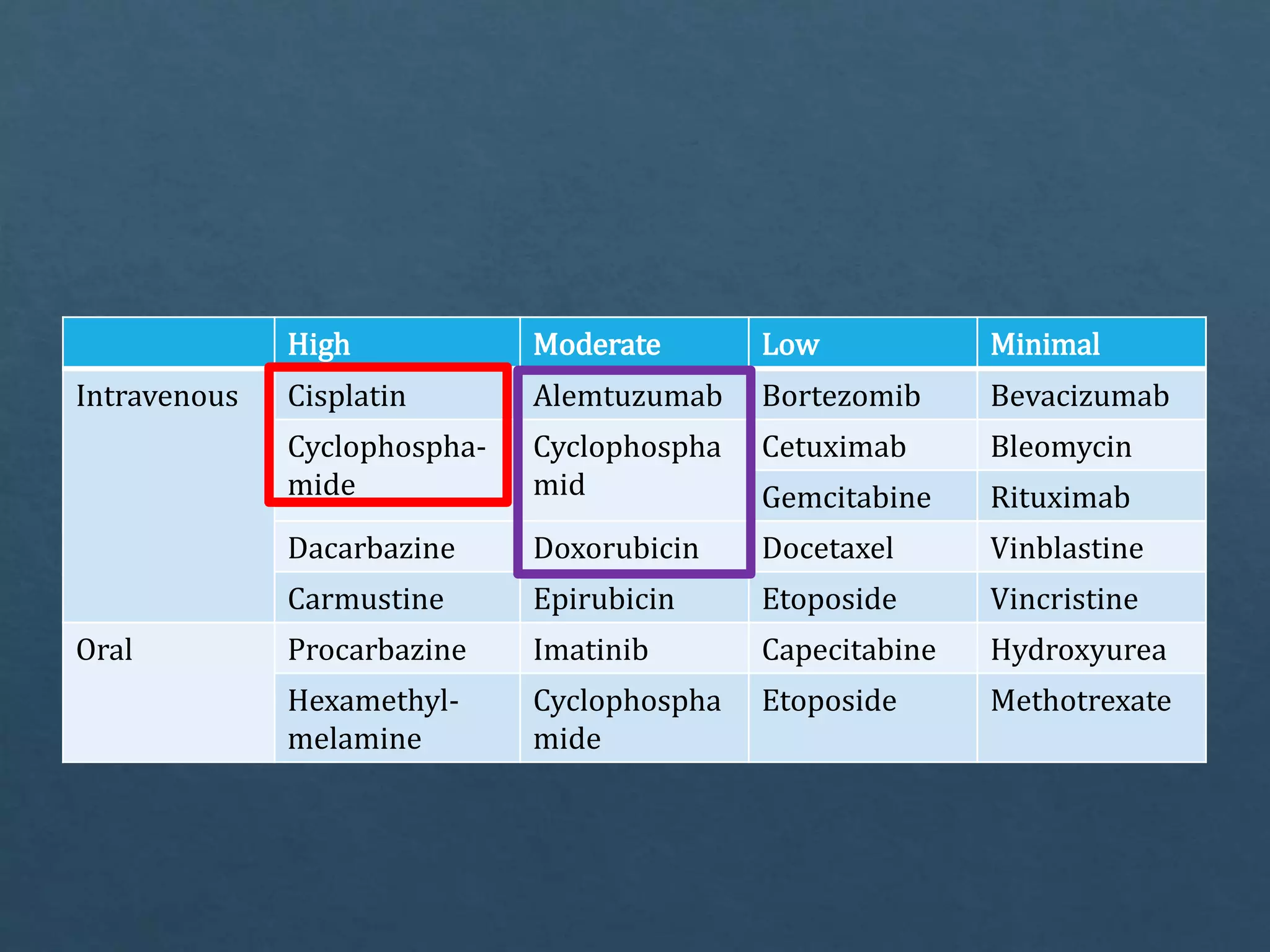
- 45. High Moderate Low Minimal Intravenous Cisplatin Alemtuzumab Bortezomib Bevacizumab Cyclophospha- mide Cyclophospha mid Cetuximab Bleomycin Gemcitabine Rituximab Dacarbazine Doxorubicin Docetaxel Vinblastine Carmustine Epirubicin Etoposide Vincristine Oral Procarbazine Imatinib Capecitabine Hydroxyurea Hexamethyl- melamine Cyclophospha mide Etoposide Methotrexate