




VERMIFORM APPENDIX.pptx
- 1. VERMIFORM APPENDIX OUTLINE • Gross Anatomy • Embryology • Histology • Pathology • Clinical Presentation • Diagnosis & Treatment
- 2. Gross Anatomy INTRODUCTION • The appendix is a narrow blind-ended tube that is attached to the posteromedial end of the caecum. • It contains a large amount of lymphoid tissue which is now recently thought to play some immunologic functions in the human body. • It is supported by the mesoappendix, a fold of mesentery which suspends the appendix from the terminal ileum.
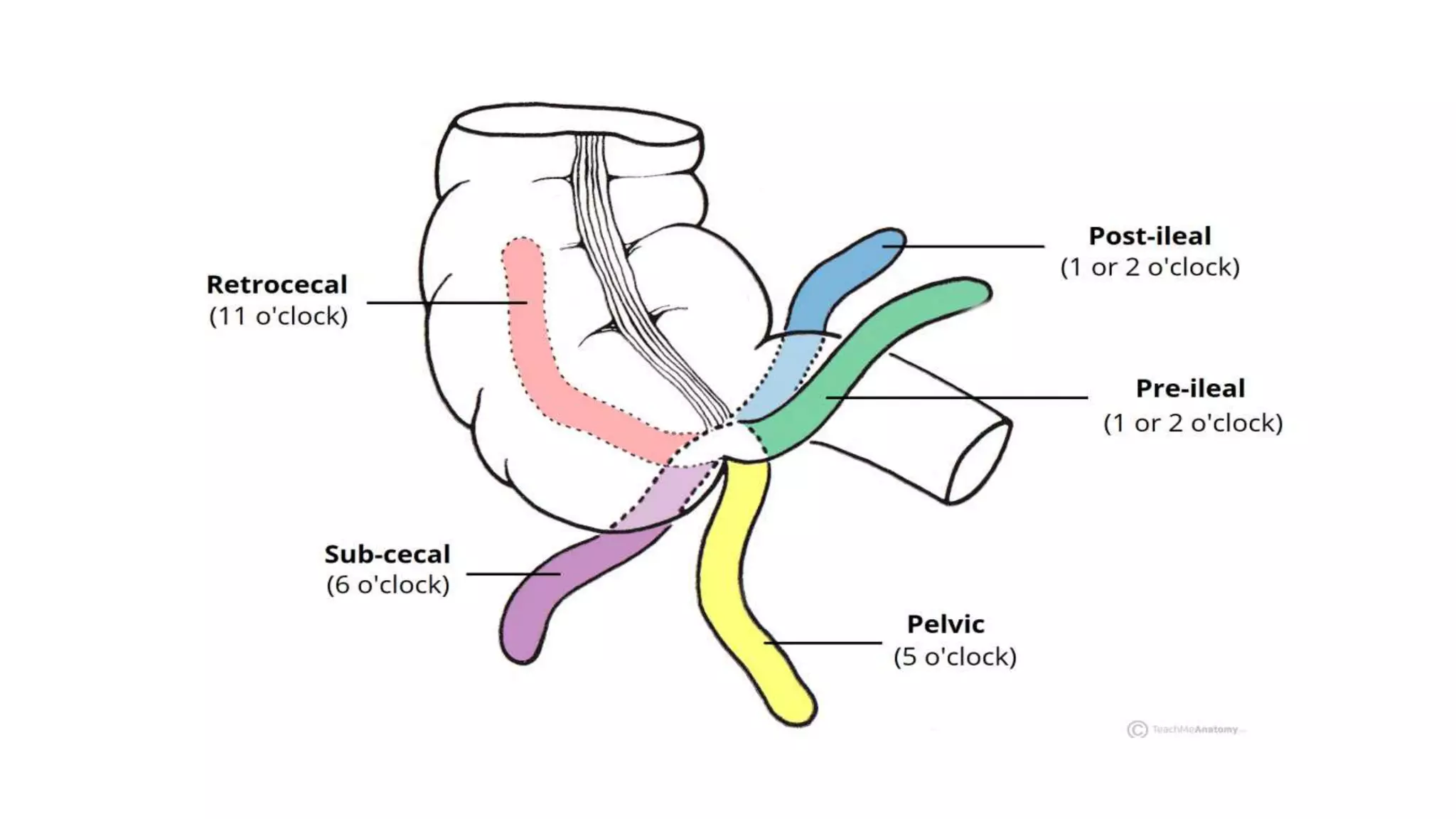
- 3. POSITIONS OF THE FREE END The position of the free-end of the appendix is highly variable and can be categorised into seven main locations depending on its relationship to the ileum, caecum or pelvis. These include: • Pre-ileal – anterior to the terminal ileum – 1 or 2 o’clock. • Post-ileal – posterior to the terminal ileum – 1 or 2 o’clock. • Sub-ileal – parallel with the terminal ileum – 3 o’clock. • Pelvic – descending over the pelvic brim – 5 o’clock. • Subcaecal – below the caecum – 6 o’clock. • Paracaecal – alongside the lateral border of the caecum – 10 o’clock. • Retrocaecal – behind the caecum – 11 o’clock. The most common position is retrocaecal.
- 5. Neurovascular Supply (A) Blood Supply: Arterial supply is from the appendicular artery which is derived from the ileocolic artery, a branch of the Superior Mesenteric Artery. (B) Venous Drainage: this is via the corresponding appendicular vein. Both are contained within the mesoappendix. (C) Nerve supply: Sympathetic and parasympathetic branches of the autonomic nervous system innervate the appendix. This is achieved by the ileocolic branch of the superior mesenteric plexus. (D) Lymphatic fluid from the appendix drains into lymph nodes within the mesoappendix and into the ileocolic lymph nodes (which surround the ileocolic artery).
- 6. Embryology • The appendix arises from the midgut. • The caecal diverticulum appears at week 6 and is the precursor of the caecum and vermiform appendix. The appendix is histologically visible by 8 weeks of gestation. • With the developmental elongation of the colon, the cecum and appendix undergo medial rotation(along with the midgut) and descend into the right lower abdomen. • As the appendix is pushed ahead of the cecum, it adopts various positions, seemingly at random. • During weeks 14 and 15, the mucosa develops lymphoid tissue, lending to its proposed function in immunity.
- 7. Histology The appendix has abundant lymphoid tissue. There are very few crypts and the lamina propria is the dominant feature of the mucosa. The appendix is composed of the four layers characteristic of the gastrointestinal tract: (a) Mucosa: • Epithelium - Simple columnar cells with microvilli. Typical cells are M-cells and goblet cells which secret mucin. • Lamina propria - comprises almost the entire mucosa. It is filled with nodules and consists of plasma cells, lymphocytes, eosinophils and macrophages.
- 8. Histology Cont. (b) Submucosa: • Nodules may extend into the submucosa (c) Muscularis Externa: • Two orthogonal layers of smooth muscle (inner circular and outer longitudinal). (d) Serosa: • Covers the outer surface of the appendix.
- 9. Pathology Depends on the degree of inflammation; 1. Simple acute appendicitis 2. Obstructive acute appendicitis: Obstruction > inflammation > oedema > pus formation and increased secretion > rise in luminal pressure > increased tension > venous stasis > arterial thrombosis > gangrene > perforation. 3. Direct pressure from faecolith > gangrene or perforation Perforation occurs in 27% of patients ( >24hours after the onset of disease). Localised or spread infection ( abscess)
- 10. Clinical Presentation History: - Pain - Nausea n vomiting - Anorexia - Bowel habits - Urinary symptoms
- 11. Clinical Presentation Cont. Examination: - Appendiceal foetor - Temp- Pulse - ? Reduced abdominal movement during respiration - RIF tenderness ( pointing, rovsings, psoas, obturator sign) - Rebound tenderness, rigidity, guarding( peritonitis) In children In elderly In pregnancy
- 12. Treatment To be discussed by the Senior Registrars on call.