

More Related Content
What's hot (20)
Viewers also liked (20)
Similar to Lumbar Drains (20)
Lumbar Drains
- 1. Lumbar Drains Elevated ICP is a contraindication for a lumbar puncture.
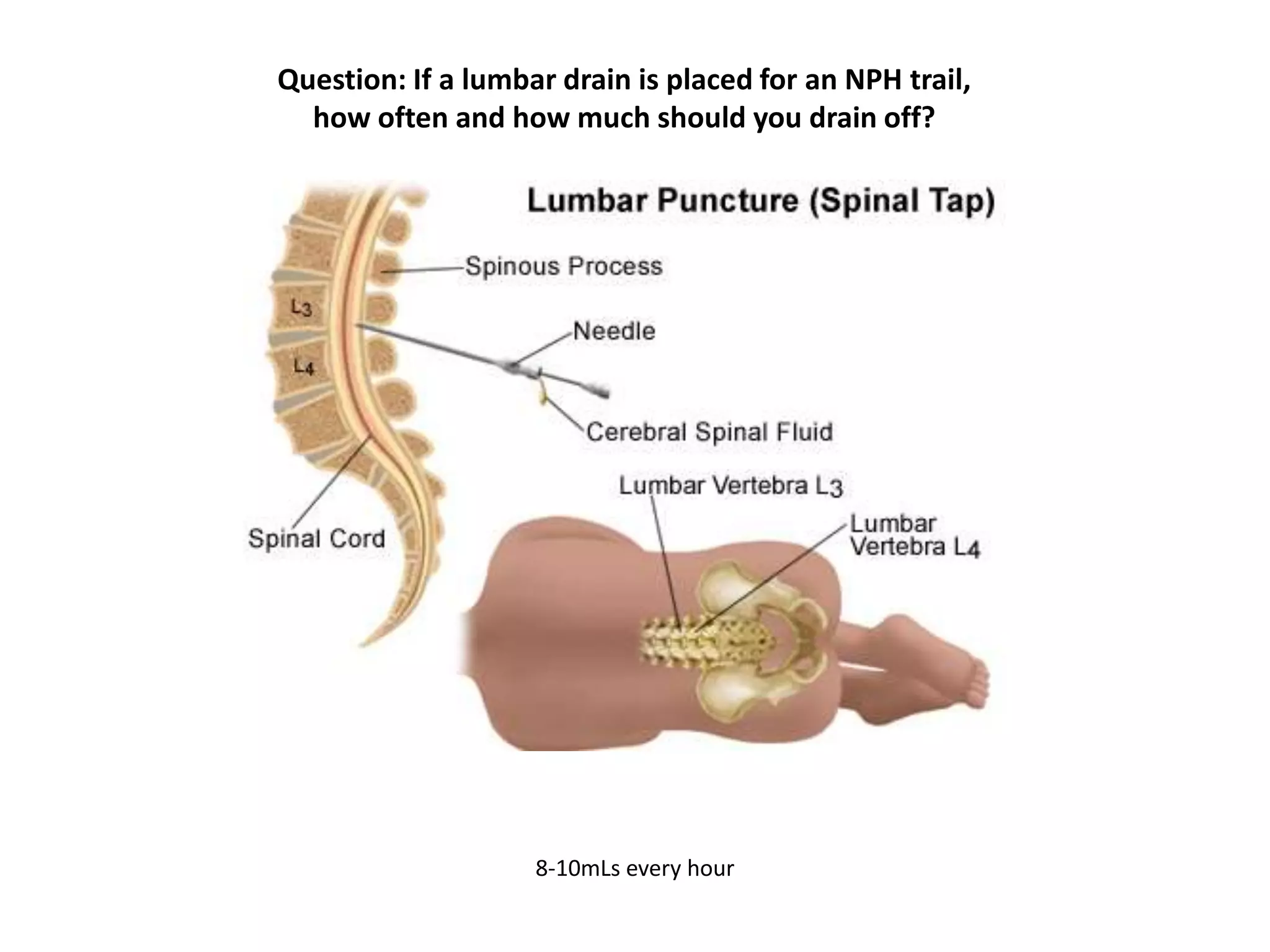
- 2. Lumbar Puncture • Kits are kept in central supply • Lumbar drain placement is a sterile procedure • Puncture sites in adults are generally between L3-L4 or L4-L5 • Punctures are general done to collect CSF Indications: • CSF analysis • Treatment of hydrocephalus caused by CSF Fistulas and Pseudotumor cerebri • Delivery of medications or contrast into the subarachnoid space – Not usually seen on our unit • Placement of a subarachnoid drain
- 3. Lumbar Puncture/Drain • Prior to placement, complete a neuro assessment and vitals • Position patient in decubitus (knee to chest) position or seated on the side of the bed leaning on a bedside table • Blood present indicates a traumatic tap • Apply an absorbent occlusive dressing that is assessed at least every 8 hours
- 4. Lumbar Drain Reportable Conditions • Respiratory depression • Changes in Level of Conciousness • Pupil changes • Motor/sensory changes • Vital sign changes • Bowel/bladder dysfunction • Headache • Persistent bleeding at the site
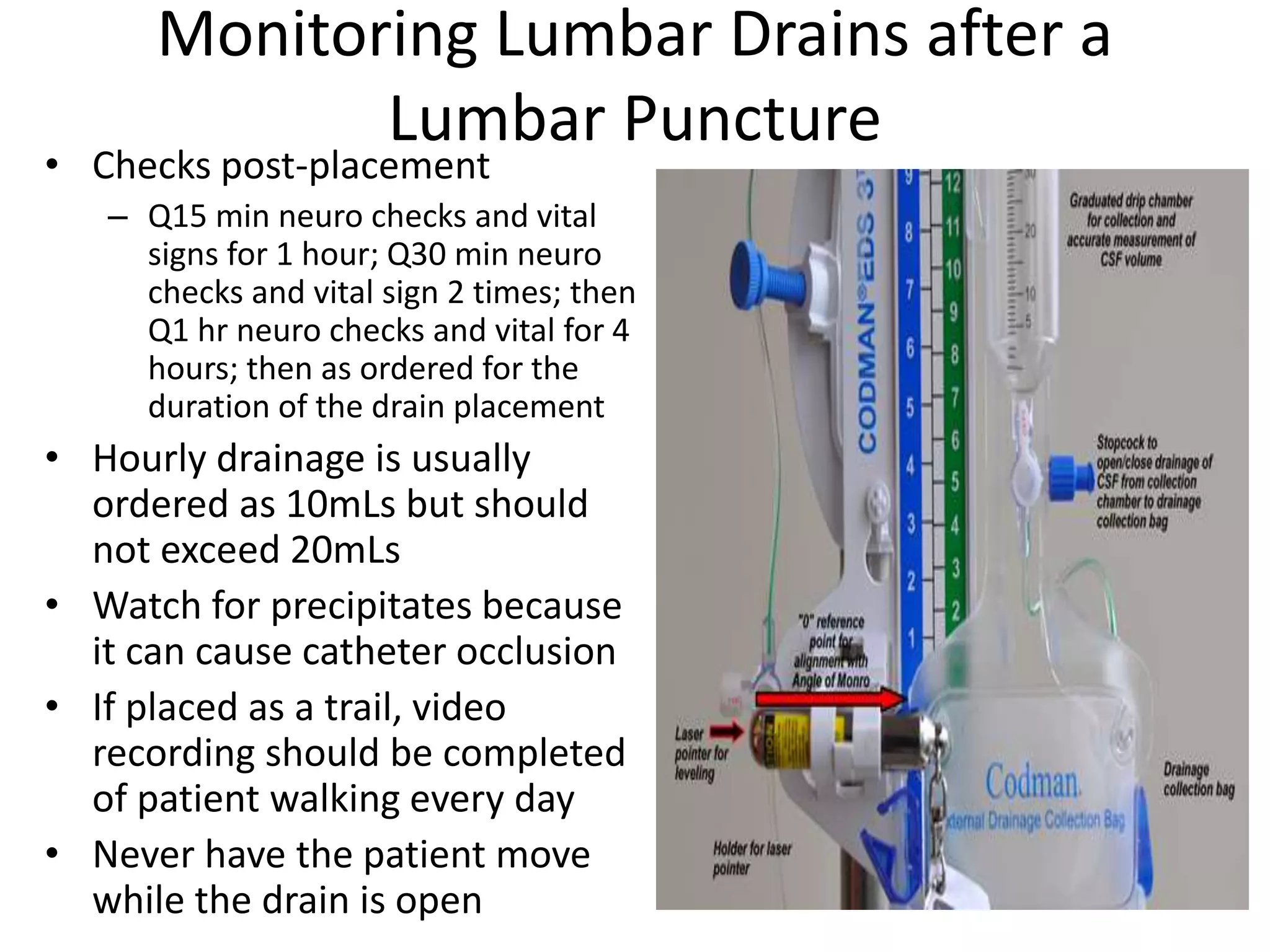
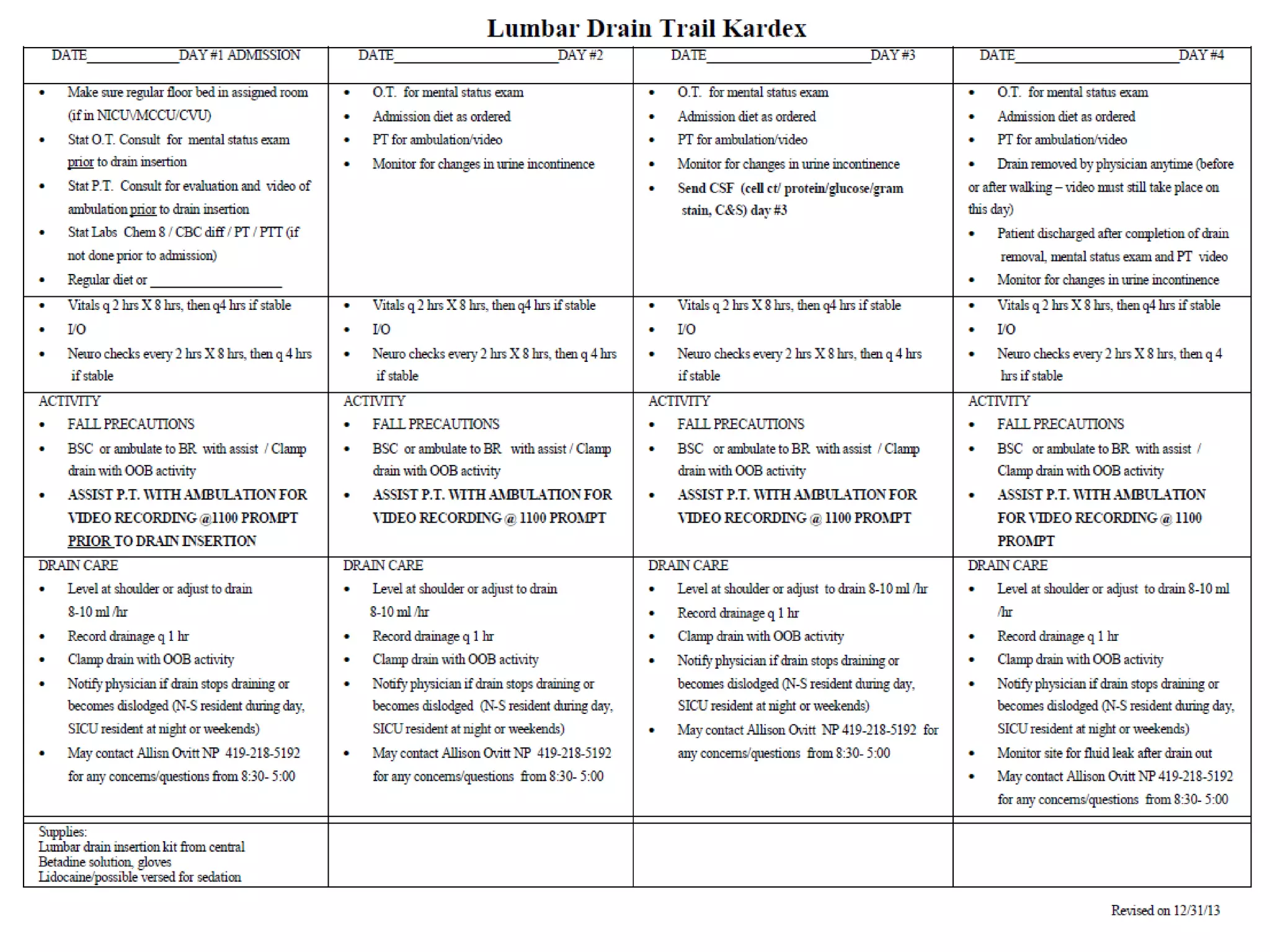
- 5. Monitoring Lumbar Drains after a Lumbar Puncture • Checks post-placement – Q15 min neuro checks and vital signs for 1 hour; Q30 min neuro checks and vital sign 2 times; then Q1 hr neuro checks and vital for 4 hours; then as ordered for the duration of the drain placement • Hourly drainage is usually ordered as 10mLs but should not exceed 20mLs • Watch for precipitates because it can cause catheter occlusion • If placed as a trail, video recording should be completed of patient walking every day • Never have the patient move while the drain is open
- 6. Lumbar Drain Trials for Normal Pressure Hydrocephalus Normal Pressure Hydrocephalous • Accumulation of CSF generally in older adults that causes ventricles of the brain to enlarge • Causes – Injury – Brain infection – No reason at all Symptoms • Gait disturbances – Mild instability to inability to stand or walk • Dementia – Loss of interest in daily activities, forgetfulness, difficulty dealing with routine tasks, and short-term memory loss • Urinary incontinence – Urinary frequency and urgency in mild cases, whereas a complete loss of bladder control can occur in more severe cases
- 7. Maintenance of a Lumbar Drain from the Competency • Every hour assess and document the color, clarity, and volume of the 8- 10ml of CSF and the patency of the system • Every 2 hours perform a comprehensive neurological and vital sign assessment and compare to baseline values. • Notify the physician if the patient experiences changes in the level of consciousness, neuro deficits, and/or a headache • Limit patient mobility, and report inability of the patient to follow the safety instructions to the physician. • Prevent dislodgement of the lumbar catheter through repeated explanation, sedation/analgesia or, as a last resort, the use of mechanical restraints. • Every 4 hours perform a complete head to toe assessment of the patient. • Assess the lumbar catheter insertion site. • Ensure the dressing covers the catheter tubing and that no kinks are present. • Reinforce the dressing when loose. If soiled call the physician. • Maintain the integrity and sterility of the closed system by keeping all connections tight. • Do not secure drainage tubing to the bed as this may dislodge the catheter if the patient moves abruptly. • Do not allow tubing to rest under the patient when he or she is side lying because it may impede CSF flow when drain is open.
- 8. CSF Specimen Collection from a Lumbar Drain • Obtain the sample using aseptic technique from the port closest to the patient. • Perform hand hygiene. Don sterile gloves, mask, and cap. • Swab the puncture port or stopcock on tubing with antimicrobial agent for three minutes (betadine, NOT Chlorahexadine) and allow drying (a minimum drying time of 3 minutes is recommended for iodine solutions). • Swab the puncture port or stopcock on tubing with antimicrobial agent for three minutes (betadine, NOT Chlorahexadine) and allow drying (a minimum drying time of 3 minutes is recommended for iodine solutions). • Document the procedure.
- 9. Changing the Drainage Bag for a Lumbar Drain • Perform hand hygiene. Don sterile gloves, mask, and cap. • Turn the stopcock closest to the bag, off to the patient to prevent the flow of CSF. • Disconnect the bag from the system; clean the disconnection site with an iodine swab for three minutes. • Cap the full bag to prevent leakage and discard it as hazardous waste. • Maintain aseptic technique. Connect the new sterile drainage bag with just enough pressure to secure but not enough to break connector. • Ensure that the stopcocks are in the correct position for drainage.
- 11. After the Lumbar Drain is Removed 2 weeks after discharge, the patient will follow up with the Neurosurgeon and if improvements are made, a peritoneal ventricular shunt will be placed.
- 12. Question: If a lumbar drain is placed for an NPH trail, how often and how much should you drain off? 8-10mLs every hour