Ect by dr asma
•Download as PPT, PDF•
11 likes•959 views
ECT involves inducing a brief, controlled seizure in patients through the application of electric currents to the brain. It has been used effectively to treat severe depression and other mental illnesses since the 1930s. The document outlines the history, machines, mechanisms of action, indications, techniques, risks, and typical treatment protocols for ECT. It explains that ECT aims to restore normal neuroendocrine and neurotransmitter system functioning through repeated seizures, and is considered very safe when administered properly by a psychiatrist.























Ect by dr asma
- 1. Electro-Convulsive Therapy (ECT) Dr.Asma A Rehman Consultant Psychiatrist
- 2. Overview • Definition • History • Machines • Mechanism of action • Indications • Technique • Unwanted effects • Summary
- 3. Definition • ECT is a procedure in which electric currents are passed through brain, intentionally triggering a brief seizure. • Formerly known as “ Electric Shock ” • Safe for all ages, with debilitating illness, and during pregnancy.
- 4. History • Introduced in late 1930’s • On basis of mistaken idea : “ Epilepsy and Schizophrenia do not occur together” • Induced fits should lead to improvement in Schizophrenia. • Initially chemically fits were induced by using Camphor or Pentylenetetrazol. • IV Camphor induced seizure in 1934 by Meduna As procedure was painful so Then started on ECT • IM pentylenetetrazol • 1st ECT in 1938 .
- 5. • 1940, curare was developed for use as a muscle relaxant during ECT • Succinylcholine, a depolarizing muscle relaxant, was introduced in 1951 • 1975 movie “One Flew Over the Cuckoo’s Nest,” with Jack Nicholson thrashing about, forced against his will to endure painful, violent seizures • In 1985, the National Institutes of Health and National Institute of Mental Health Consensus Conference on ECT endorsed a role for the use of ECT
- 6. ECT machines. • Four machines currently available are recommended by the College: 1. the Ectron Series 5A, 2. Ectonus (Electron Ltd, Letchworth), 3. Mecta SR2 and JR2 (Mecta Corp., Lake Oswego, OR) and 4. Thymatron-DGx (Somatics Inc., Lake Bluff, IL) ( Royal College of Psychiatrists, 1995).
- 7. ECT machine in LNH (ECTONUS)
- 9. Mechanism Of Action. • Neuro-endocrine system • Neuro-endocrine dysregulation Is prominent in Patients with Mental disorders for which ECT is effective. • In severely depressed patients, Adrenal glands produce too much Cortisol. • The high blood levels disrupts normal diurnal rhythm of other glandular discharges and the glands do not respond to usual feed back mechanism.
- 10. • The most prominent features of depression are distortion of functions regulated by Neuro-endocrine gland in self- adjusting feed back. • Each Seizure stimulates Hypothalamus to discharge its hormones, which causes Pituitary gland to discharge its products which then effects level of Cortisol. • The first effects of this cascade are Transitory, but repeated Seizures restore the normal interaction of HPA axis. • Feeding & sleeping becomes normal, followed by motor activity, mood , memory & thoughts.
- 11. • After some course of ECT, the return to normal Endocrine functions. • At other times, glands revert their abnormal activities, & mental disorder becomes evident again. • In these cases repeated stimulation of Hypothalamus & Pituitary by continuation of ECT restore & sustain normal glandular function & support normal mental state.
- 12. • Neuro-transmitter System. • Almost all neurotransmitters effected by ECT. • Down regulation of pot-synaptic beta adrenergic receptor • Increase post-synaptic receptor & change in pre-synaptic discharge.
- 13. Indications. • 1) Treatment of choice : • Severe depressive illness when associated with : oLife threatening illness bec of refusal of food & fluids. oHigh Suicidal risk. • 2) Considered for: • Severe Depressive illness associated with: oStupor. oMarked Psychomotor retardation. oDepressive delusions & hallucinations.
- 14. • 3) 2nd & 3rd line of treatment: • Depressive illness: o If not responsive to anti-depressant drugs • 4) Treatment of Mania: • associated with: o Life threatening physical exhaustion. o Not responded to appropriate drug treatment. • 5) For treatment of Acute Schizophrenia: • as 4th line treatment option. o After trial of 2 anti-psychotics & Clozapine was ineffective • 6) Catatonia. o Where treatment with Benzodiazepine ineffective.
- 15. • Mortality Rate. • 3-4/100,000 Treatments. • Due to General Medical conditions or General Anesthesia complications. • Contraindications. • No absolute contraindications. • Contraindications are due to anesthesia
- 16. Technique • Pre-treatment evaluation: • Complete physical examination • Dental examination • Complete Blood Picture. • Serum Urea/Creatinine/Electrolytes. • Urine Tests • Chest X-ray • ECG • CT-Scan. • MRI. • ECT Clinic: • Pleasant safe surroundings • Waiting area should separate from treatment room • Emergency equipment should be present • ETT. • Suction. • O2 supply. • Resuscitation.
- 17. • Arrival of patient: • Patient should be at ease. • Check identity • Check consent form. • Check drug sheet. • Administration of Anesthesia. • NPO for at least 5 hours. • I/V access maintained. • Attach Monitor • Give Muscle relaxant • Anesthetic agent • Hyperventilation with O2 • Bite Block. • Electrode placement and electical dose. • Managing complications. • Shift to recovery room till patient concious and stable.
- 18. Muscrainic anti-cholinergic: • Administered before anesthetic agent • To minimize oral and respiratory secretions. • Atropine 0.3-0.6 mg IM or SC 30-60 minutes before anesthetic agent OR • 0.4-1.0 mg IV 2 or 3 minutes before anesthetic • Suxamethonium Chloride 0.5-1mg/kg i/v bolus
- 19. Anesthetic agent. • Methohexital (BREVITAL) ( most commonly used) • 0.75-1mg/kg iv bolus • Thiopental (PENTOTHAL) 2-3mg/kg iv bolus
- 20. Other anesthetic agents used.
- 21. Muscle relaxant. • After onset of anesthetic effect within a minute. • To minimize risk of bone fractures and other injuries. • Succinylcholine 0.5-1 mg/kg iv bolus.
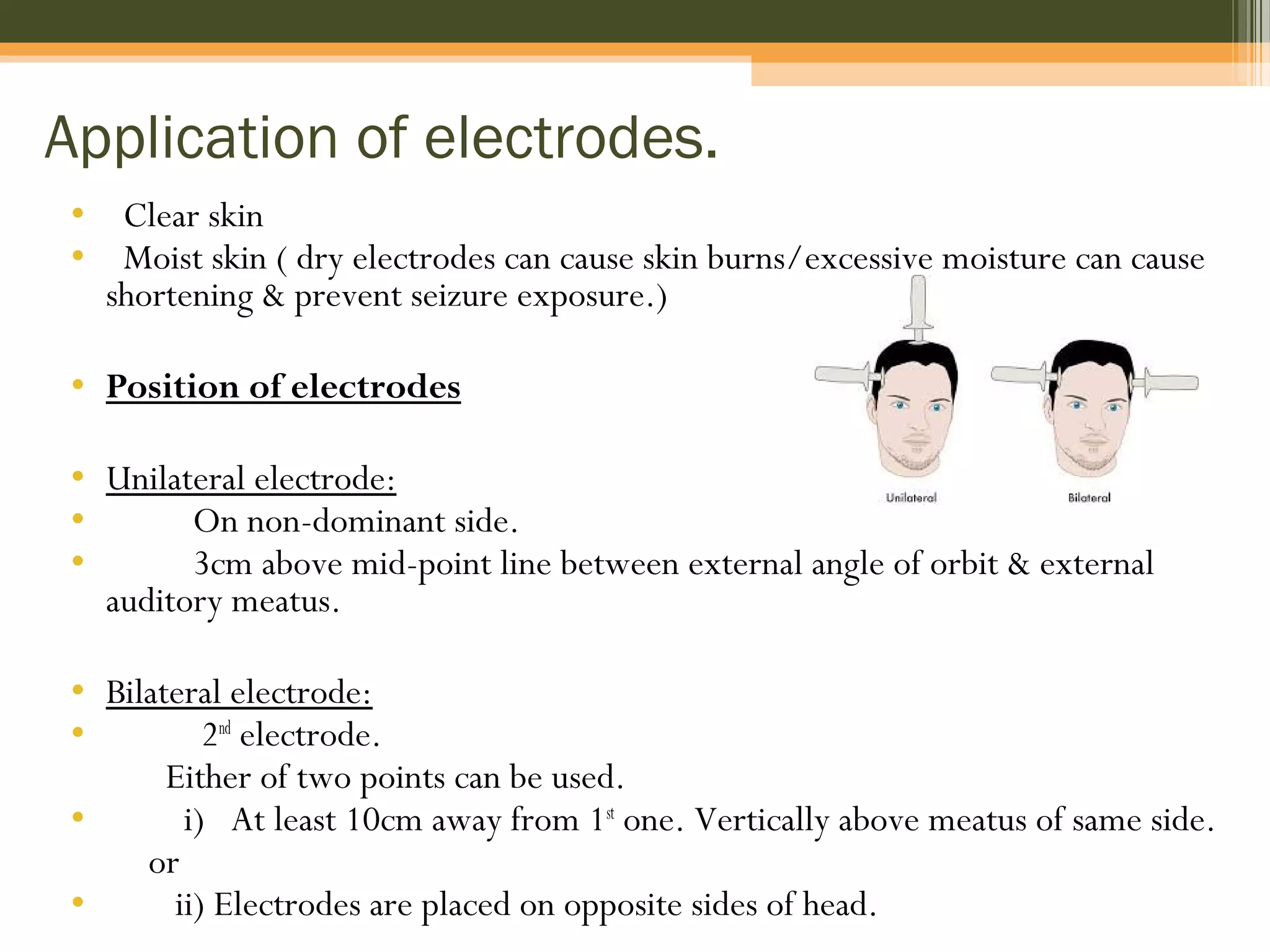
- 22. Application of electrodes. • Clear skin • Moist skin ( dry electrodes can cause skin burns/excessive moisture can cause shortening & prevent seizure exposure.) • Position of electrodes • Unilateral electrode: • On non-dominant side. • 3cm above mid-point line between external angle of orbit & external auditory meatus. • Bilateral electrode: • 2nd electrode. Either of two points can be used. • i) At least 10cm away from 1st one. Vertically above meatus of same side. or • ii) Electrodes are placed on opposite sides of head.
- 24. Electical dose. • For unilateral fixed ECT: 400 milicoloumbs • For Bilateral ECT: 100-200 milicoloumbs. • Seizure threshold increased in men. • For age <40 • Starting dose: 150 milicoloumbs. • Dose might be increased if seizure was short or absent.
- 26. Signs of seizure. 1st • Muscle of face begin to twitch & mouth drops open. Then. • Upper eyelids, thumbs & big toe jerks rhythmically for 1½ minute. • Seizure duration: 20-50seconds.
- 27. Monitoring by EEG • Many modern ECT machines now include EEG monitoring, which helps to prevent unwarranted re- stimulation, as well as to detect prolonged seizures.
- 29. Concomitant medications. • Anti-depressant & anti-psychotics decrease seizure threshold. • Benzodiazepine should be withdrawn because of anti- convulsant effect. • Valproate & lamotrigine increase threshold. • Clozapine and Bupropion should be withdrawn because associated with late appearing seizures. • Cognitive impairment when ECT given with Lithium. • SSRIs prolong seizure duration. • Lidocaine should not be administred as increase seizure threshold. • Theophylline contraindicated as increases seizure duration. • Reserpine also contraindicated as compromise respiratory and CVS during ECT
- 30. Complications. • Prolonged and tardive seizure. • Duration > 180 seconds.(APA guidelines) • > 120 seconds ( Royal College’s revised guidelines) • Status epilepticus. • Give i/v diazepam 5-10mg immediately. • Failed stimulation. • If no seizure occurred Check machine. Check electrodes. Check contact with skin. • Charge can be increased by 50% & further stimulus can be given. • Additional procedure to lower seizure threshold include Hyperventilation and • administration of 500-2000 mg iv of Caffeine Sodium Benzoate 5-10 minutes before stimulus.
- 31. Unwanted effects • Brief Retrograde Amnesia: loss of memory up-to 30 minutes after ECT. • Brief disorientation. • Headache • Muscle pain esp. jaws. • Occasional damage to teeth, tongue or lips. • Small electical burns (due to poor application of electrodes) These unwanted effects are rare if good anesthetic technique used. Other rare complications occur due to co morbid physical illness.
- 32. Memory disorder after ECT Short-Term effects Long-Term effects Retrograde Amnesia Anterograde Amnesia Loss of memory for personnel and impersonal remote events. Dec ability to learn new information.
- 33. Frequency and number of treatments • Can be given Twice a week. • In general. 3 times/week given. • Course of ECT includes 6-12 treatments. • Little response until 2-3 treatments. • If no response after 6-8 treatments , course should be abandoned. • Prevention of relapse:- • In depression high relapse rate until continuation therapy with anti-depressants. • Maintenance ECT • At reduced frequency. • Fortnightly or monthly.
- 34. Thank you •Hope it was not an ELECTRIC SHOCK for YOU
Editor's Notes
- Thyroid, Adrenal, Sex glands & Hypothalamic dysfunction are common in patients in patients with disorders in mood, thought, motor act, feeding, sleep, sex, growth & maturation.
- The most prominent features of depression are failure to eat, loss of weight, inability to sleep, loss of interest in sex, inability to concentrate thoughts & difficulties in memory are distortion of functions